


ECM Skin Boosters vs Polynucleotide Skin Boosters for Rosacea, Redness and Sensitive Skin in Singapore: 10 Things Every Patient Should Know
By Dr Law Zhi Wei, Aesthetic Doctor at The Clifford Clinic, Singapore
For rosacea, persistent redness, and sensitive skin, the choice between an ECM skin booster and a polynucleotide skin booster comes down to signal versus scaffold. A polynucleotide skin booster calms inflammation and supports repair, which suits stable reactive skin, but it is usually deferred during an active flare because micro-injection can over-stimulate a compromised barrier. An ECM skin booster, a human acellular dermal matrix (hADM) skin booster, instead replaces the structural matrix that the skin barrier is built from. Recent peer-reviewed evidence links it to lower inflammatory signalling and measurable barrier improvement. Which one is right depends on whether your skin is inflamed, barrier-weak, or both.
If you have rosacea or skin that flushes, stings, and stays red, you have probably been told a skin booster might help, then left to work out which one. In Singapore, the two most discussed injectable options for reactive skin are polynucleotide boosters and the newer extracellular matrix (ECM) boosters. Yet they are often described as if they do the same job. They do not.
This guide compares the two for the specific problem of rosacea, redness, and sensitive skin, rather than for a general glow. It explains what each one actually delivers into your skin, what the published evidence shows, when each is appropriate, and the single timing rule that matters most for inflamed skin.
The aim is a clear decision framework you can bring to a consultation, not a verdict that one product wins for everyone. For the wider picture, see our ECM skin booster treatment page and a shorter overview of ECM skin boosters, then use this article to choose between the two options for reactive skin. In many rosacea-prone patients in Singapore, the most honest answer is a sequence of both, in the right order.
On this page
- What is the real difference between an ECM skin booster and a polynucleotide skin booster?
- What is actually inside each product?
- Why is rosacea a separate conversation from ordinary dryness or dullness?
- Do polynucleotide skin boosters help rosacea, and when should they be deferred?
- What does the peer-reviewed evidence show for an ECM booster in barrier-compromised, redness-prone skin?
- Which option is more comfortable and has less downtime for reactive, sensitive skin?
- How fast does facial redness settle with each, and how long does it last?
- How does Singapore’s climate affect the choice for rosacea-prone skin?
- Which patient profiles suit an ECM booster, a polynucleotide booster, or both?
- When is a sequenced combination of the two the most honest answer?
1. What is the real difference between an ECM skin booster and a polynucleotide skin booster?
The core difference is signal versus scaffold, and it decides almost everything else.
An ECM skin booster is a generator: it places the actual building materials of the dermis, a human acellular dermal matrix, directly into the skin. A polynucleotide skin booster is a stimulator: it delivers DNA-derived fragments that signal your own cells to repair and calm down. One supplies the structure; the other sends a message to the cells that maintain it.
Rosacea-prone skin often has two problems at once: an inflammatory tendency and a physically weakened barrier. A stimulator is well-suited to the first. A generator is aimed at the second, because it adds matrix rather than relying on already-stressed cells to manufacture it.
Neither approach is inherently superior. The right tool depends on which problem is dominant, which is why the rest of this guide is organised around matching mechanisms to skin state rather than declaring a single answer.
Not all skin boosters work the same way for rosacea-prone skin. This comparison shows how an ECM (human acellular dermal matrix) skin booster and a polynucleotide skin booster differ in mechanism, comfort, timing and the type of redness each one suits.
| Factor | ECM skin booster (hADM) | Polynucleotide (PN) skin booster |
|---|---|---|
| How it works | Generator: supplies the matrix directly | Stimulator: signals cells to repair and calm |
| What it’s made of | Human acellular dermal matrix: collagen, elastin, fibronectin, laminin, glycosaminoglycans | Polynucleotide chains derived from salmon or trout DNA |
| Best-suited skin | Barrier-weak, thinning, structurally depleted | Inflamed, reactive, easily provoked |
| Effect on inflammation | Lower inflammatory signalling | Calms inflammation, supports repair |
| Comfort and downtime | Cannula or fine micro-injections; fewer entry points | Multiple shallow injections, transient bumps |
| During an active flare | Timing assessed at consultation | Commonly deferred until the flare settles |
| Onset and how long it lasts | Gradual rebuild, longer-lasting | Faster calm, shorter cycle |
| Overall recommendation | Choose when redness is barrier-led, or for longer-term skin-quality rebuilding | Choose when redness is inflammation-led and the skin is stable; often combined with the above |

2. What is actually inside each product?
Composition predicts how each behaves in sensitive skin.
An ECM skin booster is built from a human acellular dermal matrix, processed so that cells and immunogenic material are removed while the native scaffold is preserved. According to the manufacturer’s technical documentation, that scaffold is roughly 89 percent Type I collagen, with elastin, fibronectin, laminin, and glycosaminoglycans making up the remainder, delivered as sub-100 micron particles. It is a concentrated version of the matrix your barrier is physically made from.

A polynucleotide skin booster is composed of purified polynucleotide chains, long fragments of DNA usually sourced from salmon or trout. These fragments do not become structural tissue. Instead, they work biologically, calming inflammation and supporting the skin’s own repair, an anti-inflammatory effect reviewed by Squadrito and colleagues in Frontiers in Pharmacology (2017).
So one product is closer to a structural transplant of matrix, and the other is closer to a biological repair signal. That is the practical reason their best-fit patients differ, and why combining them can make sense when both problems are present.
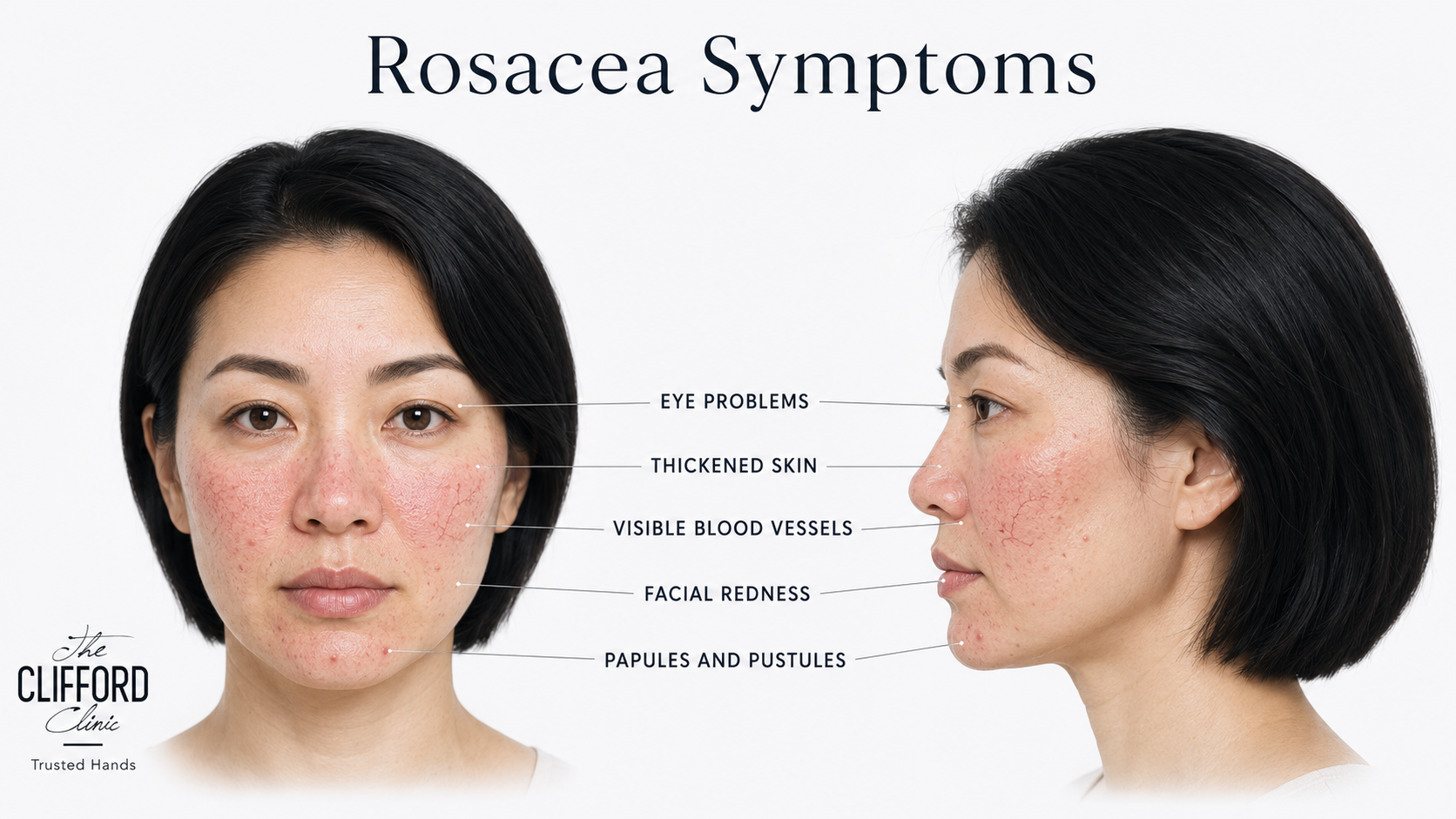
3. Why is rosacea a separate conversation from ordinary dryness or dullness?
Rosacea is barrier failure plus overactive innate immunity, not just a lack of water.
Rosacea-prone skin is characterised by a measurably weakened barrier. Studies have shown increased transepidermal water loss and lower stratum corneum hydration in both the erythematotelangiectatic and papulopustular forms, meaning the skin literally leaks water and lets irritants in more easily.
On top of that, the skin’s immune defences are overactive. An immune molecule called cathelicidin LL-37 builds up in rosacea skin, where it drives redness, flushing, and visible vessels. This pattern is described by Reinholz and colleagues and in a 2025 review in Clinical and Experimental Medicine. The barrier weakness and the inflammation feed each other: a leakier barrier switches on the inflammation, and the inflammation keeps the barrier weak.
This is why a plain hydration booster usually disappoints rosacea patients. Adding surface water does not rebuild the matrix that is failing, nor does it lower the inflammatory signalling. The treatment has to address structure, inflammation, or both, which is the axis on which these two categories differ. Where visible vessels and flushing dominate, vascular laser for rosacea and redness is often part of the same plan.
4. Do polynucleotide skin boosters help rosacea, and when should they be deferred?
Yes, for stable, reactive skin, but they are commonly deferred during an active flare.
Polynucleotide boosters have a credible anti-inflammatory rationale for rosacea. By damping inflammatory signalling and supporting cellular repair, they can help calm reactive skin, strengthen tolerance, and reduce background redness over a course of sessions. As a result, many Singapore clinics now offer them for sensitive, redness-prone skin.
The important caveat is timing. Because the treatment is delivered as multiple shallow micro-injections, introducing it into skin that is mid-flare, raw, or acutely inflamed can over-stimulate an already compromised barrier and prolong redness or bumps. Practitioners commonly wait until the skin is settled before starting, a point reflected across clinical guidance on who should avoid the treatment during active inflammation.
A polynucleotide booster is often a good fit for rosacea between flares, but it is not suitable as a rescue treatment. Timing is the most important thing for a rosacea patient to understand before requesting a polynucleotide booster injection.
5. What does the peer-reviewed evidence show for an ECM booster in barrier-compromised, redness-prone skin?
In a 2026 split-face study, the ECM approach improved the skin barrier and lowered inflammatory signalling.
The most relevant recent evidence is a 2026 split-face randomised controlled trial published in the International Journal of Molecular Sciences. It compared a human acellular dermal matrix booster against a hyaluronic acid control on opposite sides of the same face. The matrix side showed improvement in barrier-related parameters, the exact measures that are disturbed in rosacea-prone skin.
In laboratory experimentation, ECM suppressed pro-inflammatory cytokines in macrophages, suggesting an anti-inflammatory action that is mechanistically interesting for rosacea. Human acellular dermal matrix also upregulates fibroblast hyaluronic acid synthesis, linking matrix supplementation to better-hydrated, better-supported skin from within.
On safety, the 2026 clinical trial recorded no serious adverse events. In addition, longer-term studies by Yue and colleagues documented the durability and safety of acellular dermal matrix in delicate periocular tissue over years. This evidence is still early, but it is specific and peer-reviewed, which is the kind of grounding a treatment decision should rest on.

Dr Law Zhi Wei, Aesthetic Doctor at The Clifford Clinic. In my clinical experience, the patients who are most disappointed by skin boosters for rosacea are usually the ones who were given a pure hydration treatment and expected it to fix redness. It cannot, because it does not touch either the inflammation or the failing matrix underneath. When I assess a rosacea-prone face in my own practice, I am really asking one question: is this skin mainly inflamed, mainly structurally weak, or both? That answer, more than any brand, decides whether I lead with an anti-inflammatory signal, a matrix-supplying scaffold, or a planned sequence of the two. |
6. Which option is more comfortable and has less downtime for reactive, sensitive skin?
Comfort and downtime depend on how the product is delivered, which matters more in reactive skin.
Reactive skin tolerates fewer needle passes, so the delivery method counts. An ECM booster can be placed with a blunt microcannula through a small number of entry points, or with fine micro-injections. This tends to mean less surface trauma and a calmer immediate response in sensitive skin. Polynucleotide protocols typically involve many shallow injections across the face, with small bumps at the injection sites that usually settle within a day or two.
Neither has significant downtime for most patients, but the experience differs. In reactive skin, fewer punctures generally translates to a lower chance of triggering skin irritation. Comfort is one factor among several, and it is weighed at consultation alongside your flare history and skin type.
Whichever is chosen, sensitive skin does best with a conservative first session, gentle aftercare, and avoidance of heat, alcohol, and active acids for a few days, all of which we walk through individually.
7. How fast does facial redness settle with each, and how long does it last?
Stimulators tend to calm faster; generators tend to last longer.
A polynucleotide booster generally produces a relatively quick sense of calm and improved tolerance, building over a short course of sessions spaced a few weeks apart. However, the results are meaningful but comparatively shorter-lived, so maintenance comes around sooner.
An ECM booster works to rebuild the skin. It supplies and integrates matrix and prompts the skin’s own production, so the visible change in redness and skin quality tends to develop more gradually and results last longer. This is consistent with clinical trial and mechanism findings that point to durable matrix and barrier improvement rather than a transient effect.
For rosacea patients, this translates into a two-pronged approach: immediate relief from active reactivity, alongside long-term, durable barrier repair. It is this intersection of timelines that makes combining both treatments so often appropriate.

8. How does Singapore’s climate affect the choice for rosacea-prone skin?
Year-round heat, humidity, and UV keep rosacea triggers switched on, which favours durable barrier repair.
In Singapore, the climate feels like a constant trigger for rosacea. Continuous heat and humidity drive persistent flushing, and year-round ultraviolet exposure means the skin barrier rarely gets a quiet season to recover on its own.
In that setting, a treatment that durably rebuilds the matrix and strengthens the barrier has an obvious appeal, because it is working against a trigger load that does not let up. A faster-acting anti-inflammatory approach still has a role for settling reactivity, but on its own, it may need more frequent maintenance in a tropical climate.
In practice, this tilts the long-term plan for many Singapore patients toward structural rebuilding as the foundation. We then layer anti-inflammatory support around flares and seasonal peaks of heat and sun.
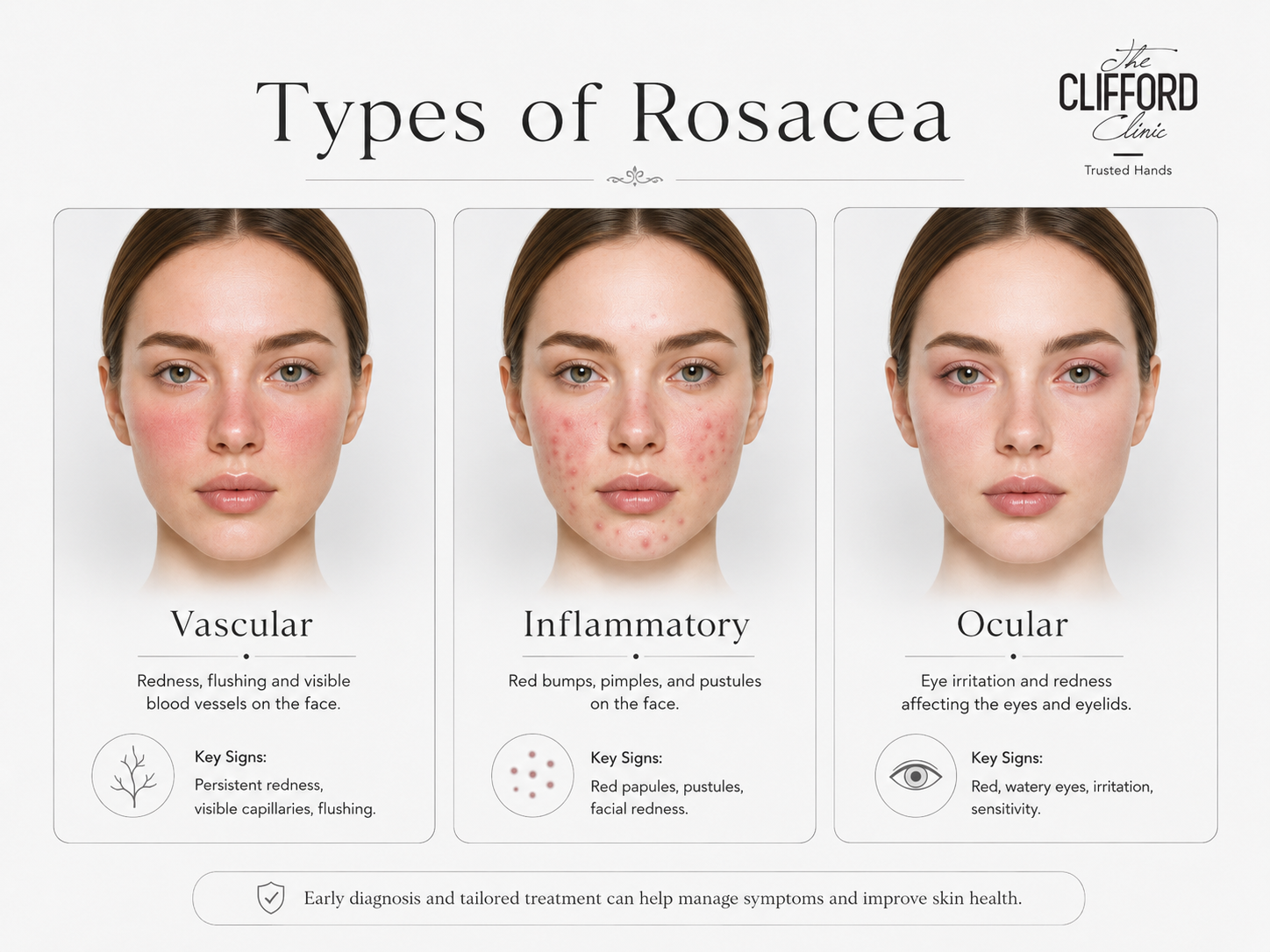
9. Which patient profiles suit an ECM booster, a polynucleotide booster, or both?
Match the mechanism to the dominant problem: inflammation, barrier weakness, or both.
Three skin profiles cover most rosacea decisions. In the first, the dominant features are inflammation and reactivity in skin whose structure is still reasonably intact, with flushing and stinging more prominent than thinning. Here, an anti-inflammatory polynucleotide approach, started once the skin is stable, is a sensible first move.
In the second profile, persistent redness sits on top of visible barrier weakness, crepey or thinning texture, and a skin that never feels robust. This is where a matrix-supplying ECM booster is most logical, because the structural deficit is what is keeping the skin reactive.
The third profile is post-procedural or post-laser redness, where the skin is recovering and needs both calming and rebuilding. Many real patients are a blend of these, which is the honest reason the answer is frequently sequencing rather than picking a side.
10. When is a sequenced combination of the two the most honest answer?
When the skin is both inflamed and barrier-weak, order matters more than choosing one.
If both problems are present, the usual logic is to calm first and rebuild second. Settling the inflammation with an anti-inflammatory approach creates a stable foundation. Supplying the matrix then strengthens the barrier, so the skin is less likely to flare in the first place.
The exact spacing, which to lead with, and how to maintain it depend on the flare history, skin thickness, and how your skin has responded to previous treatments. No fixed protocol fits every rosacea patient, and anyone promising one should be treated with caution.
This is a plan built at consultation, where the skin can be examined and the sequence tailored, rather than chosen from a price list. Pricing for any treatment is discussed at that consultation.
| Dr Law Zhi Wei, Aesthetic Doctor at The Clifford Clinic.
The combination approach is the one I reach for most often for established rosacea, and the order is deliberate. I want the skin calm and stable before I do anything that rebuilds structure, because working into an active flare tends to set patients back. What I tell patients in Singapore is that our climate does not give rosacea a break. The goal is a more resilient barrier, not a quick fix that fades by the next hot, humid month. That long view is what a tailored, sequenced plan is designed to deliver. |
Frequently Asked Questions
Can a polynucleotide booster make rosacea worse?
It can if it is done at the wrong time. Used on stable skin, it generally helps calm reactivity, but injecting into an active flare can over-stimulate a compromised barrier and prolong redness or bumps. The treatment is usually deferred until the skin is settled.
Is an ECM skin booster safe for sensitive, rosacea-prone skin?
Available evidence is reassuring. A 2026 split-face trial recorded no serious adverse events, and longer-term studies of acellular dermal matrix in delicate tissue support its safety. Suitability is still confirmed individually at consultation, especially around active inflammation.
Which skin booster is better for facial redness in Singapore?
There is no single best option; it depends on whether redness is driven mainly by inflammation, by a weakened barrier, or both. Inflammation-led redness often responds to a polynucleotide approach, while barrier-led redness suits a matrix-supplying ECM booster. Many patients benefit from a sequence of both.
Can you have a skin booster during an active rosacea flare?
Generally, it is best to wait. Most micro-injection treatments are deferred until an active flare has settled, because treating raw, inflamed skin risks making the redness worse. Your skin is assessed on the day to decide if it is calm enough to proceed.
How quickly will I see less redness?
A polynucleotide approach tends to calm reactivity relatively quickly over a short course of sessions. An ECM approach works on a rebuild timeline, so the change in redness develops more gradually and then tends to last longer.
Do ECM and polynucleotide boosters work well together?
Often yes, in sequence. Most plans calm inflammation first, then supply matrix to strengthen the barrier so the skin is less prone to flaring. Spacing and order are tailored to your skin at the consultation.
Will a hydration skin booster fix my rosacea?
Usually not on its own. Surface hydration does not rebuild the failing matrix or lower the inflammatory signalling that drives rosacea, which is why patients who only had a hydration booster are often left underwhelmed.
Is an ECM skin booster the same as a collagen-stimulating injection?
No. A collagen stimulator prompts your cells to make collagen over time, whereas an ECM booster supplies a ready-made matrix of collagen and other components directly. The difference is generating structure versus stimulating its production.
How many sessions will I need?
It varies with the treatment and your skin. Anti-inflammatory approaches are typically a short course with earlier maintenance, while matrix-based approaches are often spaced further apart with longer-lasting results. A plan is set after assessment.
Does either treatment remove visible blood vessels?
Neither is primarily a vessel treatment. Visible telangiectasia is usually addressed with a vascular laser, such as Vbeam, and skin boosters are used alongside to improve barrier strength and reduce background reactivity.
Is there downtime?
Downtime is usually minimal. Polynucleotide injections can leave small bumps that settle within a day or two, and ECM boosters placed by cannula tend to cause little surface marking. Sensitive skin is managed with gentle aftercare for a few days.
How much does treatment cost in Singapore?
Pricing depends on the plan and is discussed at consultation, in line with local advertising rules that do not permit prices to be displayed. The more useful question at the first visit is which approach, or sequence, suits your skin.
Related reading at The Clifford Clinic
- Re2O ECM skin booster at The Clifford Clinic (Dr Law Zhi Wei)
- ECM skin booster in Singapore: an overview (Dr Gerard Ee)
- The clinical evidence for ECM skin boosters
- How ECM skin boosters work: fibroblast activation and dermal regeneration
- Rosacea and facial redness treatment in Singapore
- Vbeam laser for persistent redness and visible vessels
- Rejuran polynucleotide (PDRN) skin booster treatment
Book a Consultation at The Clifford Clinic
If you have rosacea, persistent redness, or sensitive skin and you are weighing a skin booster, the most useful next step is an assessment of what is actually driving your redness. From there, a tailored plan can be built around your skin, whether that is an anti-inflammatory approach, a matrix-supplying approach, or a planned sequence of both.
To arrange a consultation with Dr Law Zhi Wei, Aesthetic Doctor at The Clifford Clinic in Singapore, contact the clinic to book an appointment. Call (65) 6532 2400, WhatsApp (65) 8318 6332, or email thecliffordclinic@gmail.com. The Clifford Clinic is at 50 Raffles Place, #01-01 Singapore Land Tower, Singapore 048623 (Exit B, Raffles Place MRT). Pricing and protocol are discussed individually at that visit.
References
- Lee YI, et al. Split-face randomised controlled trial of a human acellular dermal matrix (Elravie Re2O) skin booster versus hyaluronic acid control. International Journal of Molecular Sciences. 2026. PubMed 41828422; PMC12985180.
- Liu X, Sun Y. Human acellular dermal matrix upregulates fibroblast hyaluronic acid synthesis via the JAK2/STAT3 pathway. RSC Advances. 2020. PubMed 35518338.
- Yue B, et al. Long-term safety and outcomes of acellular dermal matrix in periocular augmentation. Aesthetic Plastic Surgery. 2018. PubMed 30097671.
- The role of skin barrier and immune abnormalities in the pathogenesis of rosacea. Clinical and Experimental Medicine. 2025. PMC12553588.
- Reinholz M, Ruzicka T, Schauber J. Cathelicidin LL-37: an antimicrobial peptide with a role in inflammatory skin disease. 2012. PubMed 22577261.
- Skin barrier in rosacea: transepidermal water loss in erythematotelangiectatic and papulopustular subtypes. Anais Brasileiros de Dermatologia.
- Squadrito F, et al. Pharmacological activity and clinical use of PDRN. Frontiers in Pharmacology. 2017. PubMed 28367125.
- Two AM, Wu W, Gallo RL, Hata TR. Rosacea: Part I and Part II, pathogenesis and management. Journal of the American Academy of Dermatology. 2015.
- L&C Bio. Elravie Re2O product monograph: 150 mg human acellular dermal matrix, sub-100 micron particle size, AlloClean Technology decellularisation, composition profile. Manufacturer technical documentation.