


ECM Skin Booster in Singapore: Things Every Patient Should Know About ECM skin booster in 2026 (A Doctor’s Complete Guide)
Written by Dr Law Zhi Wei
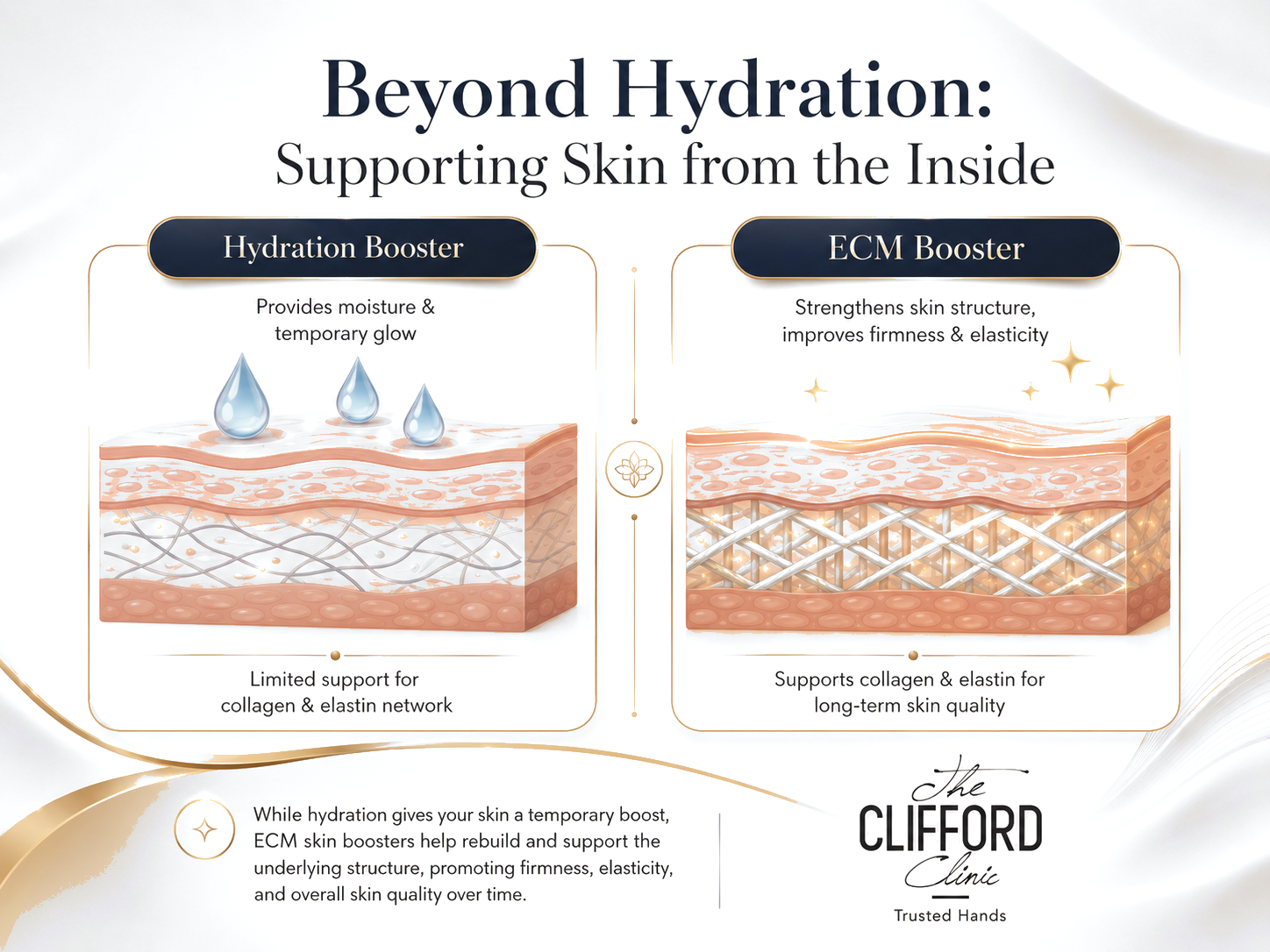
Every aesthetic patient in Singapore eventually arrives at the same realisation: hydration alone is no longer enough. By the late twenties, the structural fabric beneath your skin starts thinning. By the mid-thirties, the rate of decline outpaces what any topical or hyaluronic acid booster can compensate for. Skin still looks healthy in passing photographs, but it stops bouncing back the way it used to. The pores deepen. The texture roughens. Makeup catches on patches it never used to. This is not collagen loss in isolation. It is the slow erosion of a microscopic scaffold called the extracellular matrix, or ECM, and it is the central problem that a new generation of injectable, the ECM skin booster, was built to solve.
Elravie Re2O is a clinically substantiated ECM skin booster currently available in Singapore. It is a micronised human acellular dermal matrix, abbreviated as hADM, supplied by the Korean biotech L&C Bio, and it works in a fundamentally different way from any skin booster that came before it. Where Profhilo hydrates, PDRN signals, and PLLA stimulate, ECM skin booster does something none of them can do: it physically supplies the building blocks of the dermal matrix back into your skin, so your fibroblasts have something real to rebuild onto.
Having administered ECM skin booster at The Clifford Clinic over the past year, patients have asked us numerous questions about ECM skin booster. This is the complete patient guide for any patient who is considering an ECM skin booster could read before their first consultation. It is structured as 20 numbered sections, each one answering a specific question a patient has asked, with citations to the published clinical literature where the answer rests on data rather than opinion. It is long. Most articles on this topic are not long enough.
This is the comprehensive, long-form review. Dr Gerard Ee has separately published a shorter introductory article on ECM skin boosters at The Clifford Clinic. The guide you are reading now is the deeper companion to that piece. Where Dr Ee’s article covers the broad ECM skin booster category, the article you are reading goes considerably further: it focuses specifically on ECM skin booster, works through the published clinical evidence in detail, compares the product directly against every relevant alternative in the Singapore market, and walks through what an actual session at The Clifford Clinic looks like. The two articles are designed to be read together. Start with Dr Ee’s overview if you want the brief introduction, then return here for the definitive reference.
An ECM skin booster is not a moisturiser, a filler, or a collagen stimulator. It is something else.
It is a generator, not a stimulator.
An ECM skin booster is an injectable treatment that delivers a micronised powder of human acellular dermal matrix into the mid-dermis of the skin, providing a physical scaffold of collagen, elastin, and other extracellular matrix proteins that the body integrates as its own tissue. Three categories of injectable share the “skin booster” name, and none of them work the way an ECM booster works. A hyaluronic acid booster like Profhilo, Belotero Revive, or Juvederm Skinvive adds water and improves surface dewiness. A polynucleotide booster like Rejuran sends repair signals derived from salmon DNA, asking the skin to fix itself. A collagen stimulator like PLLA or PDLLA plants polymer microparticles that provoke the fibroblasts into making more collagen over months.

ECM skin booster does none of these things. It supplies the actual matrix material directly. The scaffold integrates with your existing tissue, the fibroblasts migrate into it, and the body remodels it as its own dermis over the following three to six months. This is what the regenerative dermatology literature refers to as a generator approach rather than a stimulator approach, and it is the reason the category has been described in clinical writing as a fourth-generation skin booster. The first generation hydrated, the second and third signalled and stimulated. The fourth supplies the substrate itself.
The extracellular matrix, not collagen alone, is what actually makes skin look young.
Collagen is just one strand in a much larger fabric.
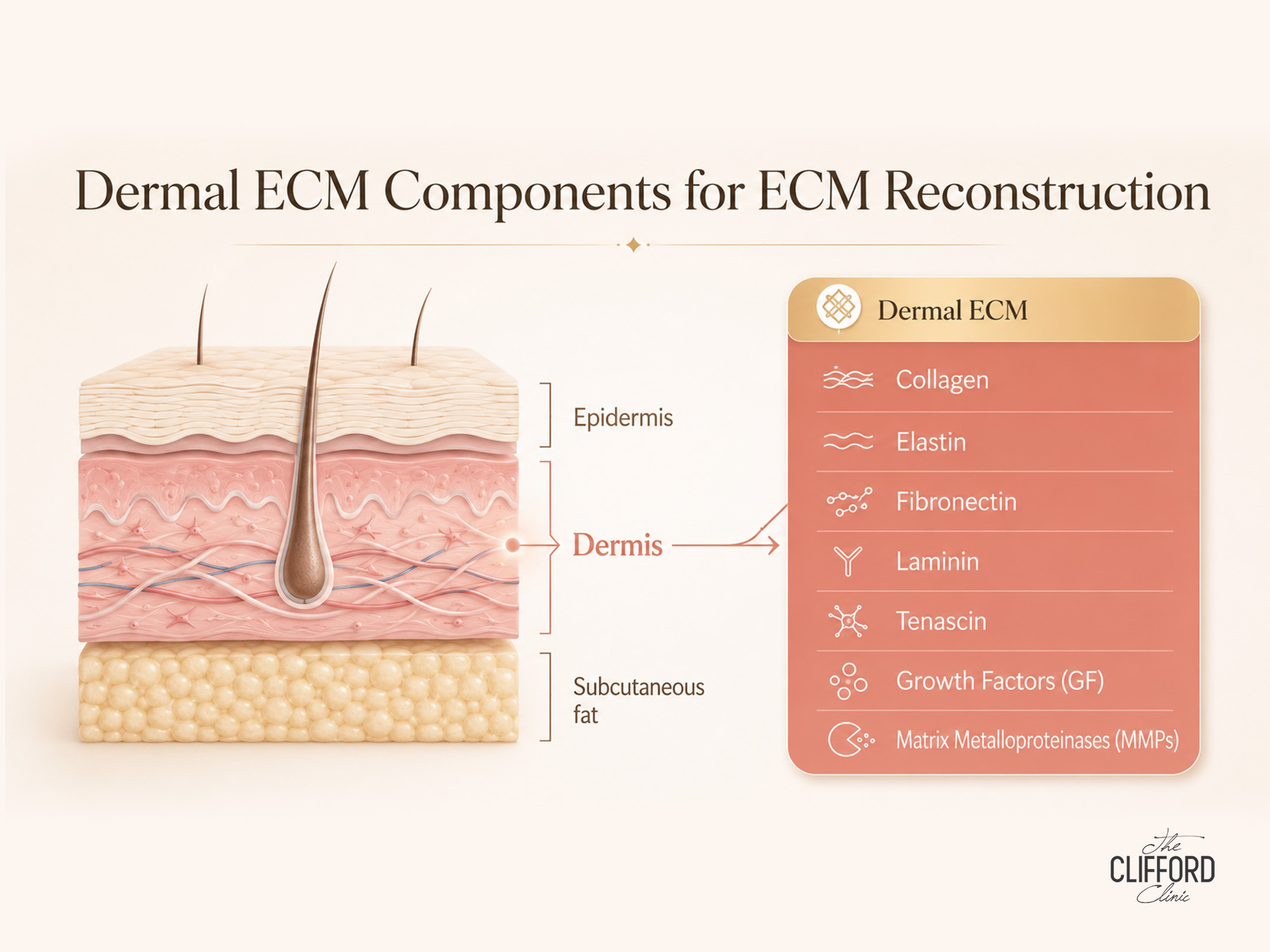
Most patient education on skin ageing focuses obsessively on collagen. Collagen is important, but the moment you isolate it from its environment, you lose the actual mechanism that holds skin together. The extracellular matrix is the three-dimensional protein lattice that lies between skin cells and provides the architecture for everything else. Collagen fibres are woven into it. Elastin coils are tethered to it. Hyaluronic acid and proteoglycans saturate it with water. Fibronectin and laminin anchor cells to it. Tenascin modulates how the cells respond to mechanical stress. Growth factors are held in reserve within it. Without this surrounding lattice, fibroblasts lose their cues and stop producing youthful protein patterns.
Research summarised by Fisher and colleagues in the Journal of Investigative Dermatology, and reinforced in Shin and colleagues’ review on the molecular mechanisms of dermal ageing, frames skin ageing as a failure of the matrix environment first, and a failure of fibroblast output second. When the ECM degrades, fibroblasts inside it receive weaker mechanical signalling and shift toward an aged, dysfunctional state. They produce less collagen, less elastin, and less hyaluronic acid, even when the cells themselves are still alive. The downstream consequences are the visible features patients describe at consultation: enlarged pores, fine lines, thinning skin, slower wound healing, dullness, and that intangible quality of skin looking tired even when the patient is rested.
ECM skin booster works because it physically restores what your skin has already lost.
Real tissue, processed, sterilised, and made injectable.
ECM skin booster is composed of finely milled human acellular dermal matrix, sourced from screened donor tissue, processed through a multi-step decellularisation protocol that removes all cells, DNA, and lipid content while preserving the native protein scaffold. The remaining powder is approximately 89 percent Type I and Type III collagen, 7.6 percent other ECM components including fibronectin, laminin, tenascin, and native growth factors, 3 percent elastin, and 0.4 percent glycosaminoglycans including hyaluronic acid. These numbers come directly from the L&C Bio product specifications and have been independently verified in the recently published clinical literature on injectable particulated hADM.

What matters about that composition is the proportion. This is not a synthetic mimic of one ECM ingredient. It is the actual ratio of proteins found in real human dermis, presented in micronised form so that it can pass through a fine injection needle and disperse across the mid-dermis. When your doctor injects it, your tissue receives a small but biologically complete copy of the dermal matrix you have been losing since your late twenties. The body recognises it, accepts it, and begins to remodel it as its own. This is the foundational reason why an ECM skin booster does what hydration boosters and stimulator boosters cannot do. The patient does not have to wait for fibroblasts to manufacture missing components. Some of those components arrive in the syringe.
AlloClean Technology and L&C Bio are the reason this product can exist at all.
Source tissue and processing fidelity decide everything.
Not every acellular dermal matrix product on the market is created equal. The integrity of the ECM scaffold depends entirely on how the source tissue is processed, and aggressive processing can fragment the very proteins the product is supposed to deliver. L&C Bio’s proprietary AlloClean Technology was developed specifically to address this trade-off. The protocol removes cellular DNA and lipid content to a level that minimises immunogenic risk, but stops short of the harsh chemical and thermal steps that would denature the collagen and elastin fibres. The result is a powder that retains the native three-dimensional pattern of ECM proteins rather than a collection of broken fragments.
L&C Bio is not a small or speculative manufacturer. It is the dominant ECM and tissue engineering company in Korea, holds roughly half of the domestic market in this category, has supplied approximately 1.72 million units across hospitals and dermatology clinics, and operates under American Association of Tissue Banks accreditation, with FDA tissue listing and Korean MFDS registration. More than one hundred papers in the Science Citation Index database reference the company’s ECM platform. This regulatory pedigree matters because tissue-derived products in Singapore are subject to a separate regulatory framework under the Health Sciences Authority known as CTGTP, which requires thirty-year traceability records of every batch and lot used in patients. A product without this paperwork cannot legally be administered.
The mechanism unfolds in three phases, not all at once.
Scaffold first, migration second, integration third.
When ECM skin booster is injected into the mid-dermis, three things happen in sequence. The first phase is immediate. The micronised matrix fills the microscopic voids in the existing dermal lattice, almost like spackle, finding gaps in a wall. This is why a small subset of patients notice a fine improvement in skin texture and a subtle smoothing within the first week. The improvement is structural, not hydration-driven, and it precedes any of the cellular activity that produces the longer-term result.
The second phase begins within the first two to four weeks. Fibroblasts, the dermal cells responsible for producing collagen, elastin and hyaluronic acid, migrate into the new scaffold. The matrix gives them something to grip and pull on, which restores the mechanical signalling cues they need to function. Once anchored, the fibroblasts begin depositing fresh proteins onto the scaffold. They also upregulate growth factor signalling, including fibroblast growth factor, vascular endothelial growth factor, insulin-like growth factor, and transforming growth factor beta. Liu and Sun demonstrated in a 2020 paper in RSC Advances that hADM contact activates the JAK2 and STAT3 signalling pathway, which in turn upregulates fibroblast hyaluronic acid synthesis. This is one of the mechanistic explanations for why the hydration effect of ECM skin booster persists for many months rather than washing away within weeks.
The third phase is the long remodelling tail, which runs from roughly three months to six months after each session. The body treats the deposited matrix as its own tissue and reinforces it with native collagen and elastin. Dermal density rises. Elasticity returns. The skin barrier improves. By the time the patient reaches the end of an initial three-session course, the cumulative effect is a measurable structural change rather than a temporary cosmetic one. This is the timeline that the published clinical trial data confirms, which is described in the next section.

Dr Law Zhi Wei, Aesthetic Doctor I want to address the question I get asked most often after a patient reads the Lee paper. “Does it actually work in real patients, outside a clinical trial setting?” My answer is yes, but with two caveats. First, the trial was conducted in twenty participants over twenty weeks, which is a small sample. The effect size was large enough to reach statistical significance across multiple skin parameters, which is uncommon for an injectable trial of that size, but it does mean we will need follow-on studies in larger and more diverse cohorts before the data is as mature as, say, the hyaluronic acid literature. Second, the technique-dependent aspects of this treatment are real. Reconstitution timing, particle dispersion, injection depth and aliquot size all influence the clinical outcome more than they do for a pre-mixed hyaluronic acid booster. The outcomes at The Clifford Clinic have closely tracked the trial results when those technique variables are kept tight. |
ECM skin booster versus PDRN: same skinbooster category, very different biology.
Material delivery on one side, repair signalling on the other.
This is the comparison I have to clarify in almost every consultation, because both products are loosely described as Korean skin boosters in the Singapore beauty press, and patients arrive assuming they are interchangeable. They are not. PDRN’s active ingredient is polynucleotide, a short-chain DNA fragment derived from salmon testes, and its mechanism is signalling. The fragments interact with cell-surface receptors and prompt fibroblasts to upregulate repair-state behaviour, which is particularly useful in patients with thin, reactive or barrier-compromised skin. ECM skin booster’s active ingredient is micronised hADM, and its mechanism is material delivery. The matrix arrives in the dermis as physical substrate. The fibroblasts integrate with it and rebuild onto it.

The practical implication is that the two products are best understood as complements rather than competitors. A patient with rosacea, sensitive reactive skin, or post-laser barrier dysfunction may benefit more from PDRN in the early phase of treatment, where the signalling-driven anti-inflammatory effect is doing the heavy lifting. A patient with visible structural decline, enlarged pores, dermal thinning, photoaged skin, or chronic dullness that has not responded to hyaluronic acid boosters tends to benefit more from ECM skin booster, where the structural deficit is the underlying problem. Many of the most refractory cases at The Clifford Clinic, for example chronic redness combined with photoageing, ultimately end up on a hybrid plan that uses both.
ECM skin booster versus Profhilo: hydration is not the same as structure.
Water glow does not rebuild scaffold.
Injectable HA is one of Singapore’s most popular injectables, and for good reason. It is a hybrid hyaluronic acid formulation with both high and low molecular weight HA fractions. It spreads widely after injection, it produces a visible hydration and dewiness effect within four weeks, and the safety profile is excellent. What Profhilo does not do is rebuild ECM structure. Its active ingredient is hyaluronic acid, which is one component of the matrix, not the matrix itself. Hyaluronic acid is excellent at binding water and producing a smooth surface appearance. It is not a structural scaffold.
The decision between ECM skin booster and Profhilo therefore comes down to which problem the patient is actually solving. If a patient walks in with mild dehydration, surface dullness, and skin that looks tired only late in the day, Profhilo is often the appropriate choice, and ECM skin booster is overkill. If a patient walks in with visible scaffold loss, deeper textural irregularity, enlarged pores, and the impression that other hydration boosters have stopped delivering meaningful improvement, Re2O is the appropriate choice, and Profhilo on its own will plateau. The two are layered together in a meaningful share of patients we treat at The Clifford Clinic, because hydration and structure are complementary rather than mutually exclusive outcomes.
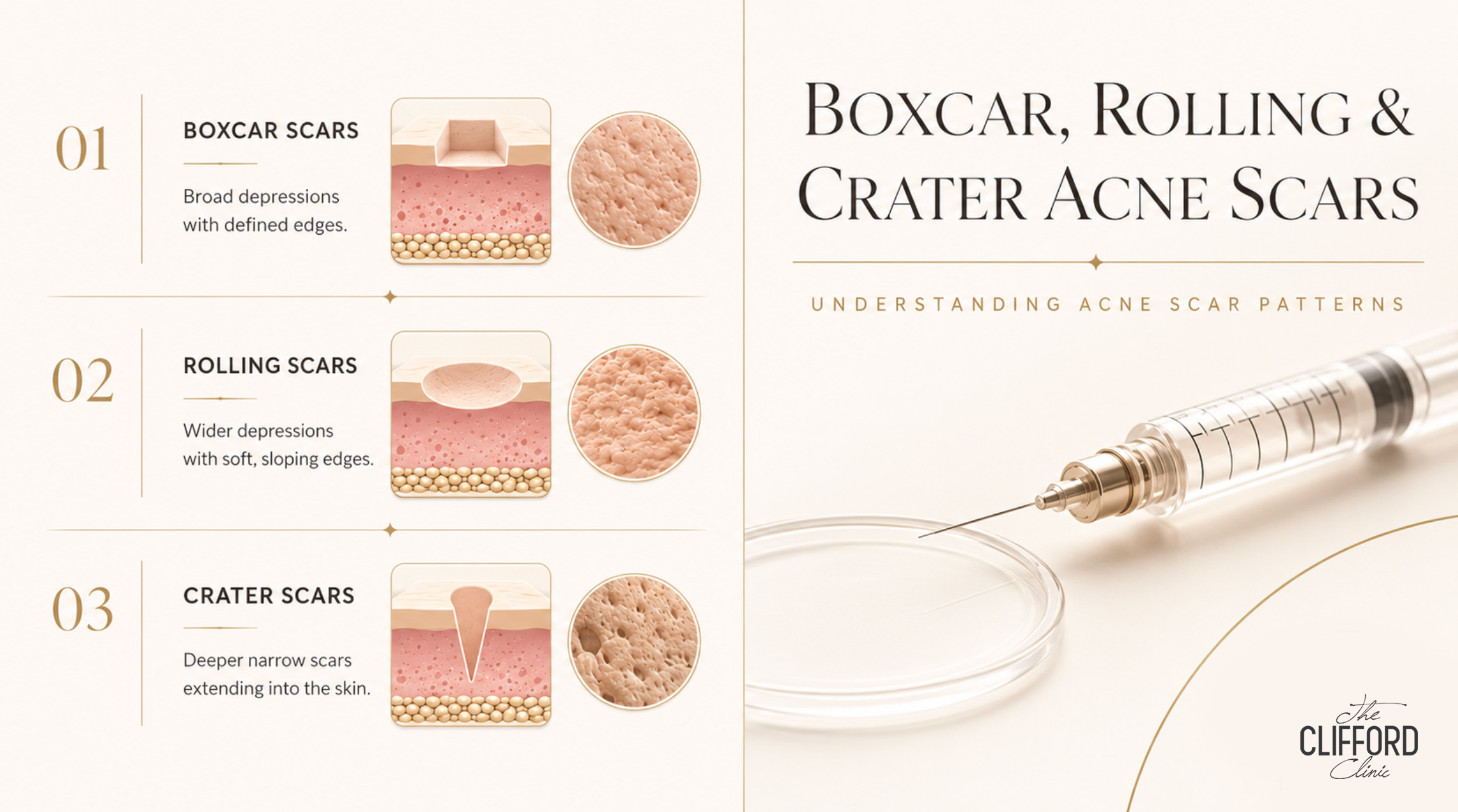
ECM skin booster versus hyaluronic acid fillers for atrophic acne scars: filling a hole is not the same as healing it.
Volume restoration does not equal tissue repair.
Patients with atrophic acne scars often arrive having tried a small hyaluronic acid filler in the scar bed. The filler does what it is designed to do: it lifts the depression mechanically and restores volume. The improvement is immediate and often dramatic in photographs, which is why it is a popular short-term solution. But it does not address the underlying tissue defect. Atrophic acne scars are areas of damaged, fibrotic dermis where the collagen architecture has been disrupted by chronic inflammation. The matrix in that scar bed is fundamentally different from the surrounding healthy skin, and a bolus of HA filler does not change that biology.
ECM skin booster approaches scarring from the other direction. Instead of lifting the depression with a volumising material, it supplies actual matrix into the scar tissue. Over the three to six month remodelling window, the fibroblasts in the scar bed have something to migrate onto and rebuild against. The improvement is slower and less photogenic than a filler, but it acts on the underlying tissue defect rather than masking it. In our clinical experience at The Clifford Clinic, the strongest results for atrophic acne scars come from combining a structural ECM approach like ECM skin booster with appropriate fractional resurfacing, subcision where indicated, and selective HA filler only in scars where the depression is genuinely volume-deficient rather than fibrotic.
ECM skin booster versus Sculptra and Juvelook: the generator versus stimulator debate.
Direct supply on one side, indirect provocation on the other.
Collagen stimulators like Sculptra (poly-L-lactic acid), Juvelook (polydioxanone-based) and Radiesse (calcium hydroxylapatite) all work through indirect provocation. They place a polymer microparticle in the dermis and rely on the fibroblasts to respond by producing more collagen over months. This is not a flawed approach. Sculptra has decades of safety data and excellent results in the right patient. But it depends entirely on the fibroblasts’ ability to mount a robust response, which declines with age, and on the patient having enough functional matrix substrate around the polymer to support that new collagen deposition.
ECM skin booster is the opposite philosophy. It supplies the matrix material directly, then lets the fibroblasts integrate it. The two approaches converge clinically in the patient who has both structural decline and a still-responsive fibroblast population, where either treatment will produce a meaningful result. They diverge in two specific patient groups. In older patients with reduced fibroblast reserve, the direct supply approach of ECM skin booster tends to outperform a pure stimulator. In younger patients with mostly intact matrix and a need for additional structural support over a long maintenance horizon, a stimulator may be the more appropriate first choice.
CellREDM versus ECM skin booster: not all hADM products are equivalent.
Particle size, source pedigree, and clinical evidence all differ.
CellREDM is the other significant injectable hADM product circulating in the Singapore and regional aesthetic market. At first glance it looks like a direct equivalent to ECM skin booster, and both products fall into the ECM skin booster category, but several practical differences matter for patient selection. Particle size, reconstitution protocol, manufacturer regulatory pedigree, and the depth of published clinical evidence differ between the two products. ECM skin booster sits on the larger L&C Bio platform with the published 2026 split-face RCT and the longer track record across Korean clinics. CellREDM has its own clinical observations and a finer particle profile that some clinicians find easier to disperse with smaller-gauge needles, but its peer-reviewed evidence base is currently thinner.
I do not have a categorical preference between the two products. The patient who presents at The Clifford Clinic is matched to the product whose particle behaviour and clinical fit suit their skin condition and treatment plan, and the manufacturer’s traceability and accreditation documentation is the non-negotiable filter that determines which products we will administer at all.
The right candidate for ECM skin booster is not defined by age alone.
Structural deficit is the relevant criterion, not the birthday.
I am cautious about age cutoffs for any aesthetic injectable, but particularly for ECM skin booster. The category is most often appropriate in patients with visible ECM deficit, which most commonly emerges in the mid-thirties and accelerates from the early forties onward, but the actual criterion is the dermal condition rather than the calendar. I have treated late-twenties patients with significant ECM loss driven by chronic UV exposure, smoking, sleep debt, and a long history of harsh topical use. I have also declined to treat patients in their fifties whose skin still has a dense, well-organised matrix and whose primary concern would be more efficiently addressed by a targeted laser or a hyaluronic acid booster.
The clinical signs I look for include enlarged pores that have not responded to topical retinoids or chemical peels, a soft and yielding skin texture on palpation, fine static lines that persist when the face is at rest, photo-textured surface dullness on visualisation, and a history of treatments that have plateaued at the hydration level without progressing to the structural level. Contraindications include active skin infection in the treatment zone, recent inflammatory flare such as untreated cystic acne or active rosacea, current pregnancy or lactation, anticoagulant therapy unless cleared by the prescribing physician, and any history of severe allergic reaction to injectable products. Patient selection is one of the most important things a clinic can get right with this product, and I will not start a course in any patient where the clinical indication is borderline.

Singapore’s climate matters more than most patients realise.
Year-round UV is the most underrated driver of ECM degradation in Asia.
Singapore’s equatorial climate produces UV index readings that rival Australia’s most intense summer days, and it produces them every month of the year rather than seasonally. The cumulative impact on dermal collagen and elastin is severe, even in patients who consider themselves diligent about sunscreen. The clinical features I see most often as a result are a particular pattern of photoaged dryness, surface roughness, dullness that does not respond to moisturisers, and a flat, dehydrated finish that worsens despite hydration boosters. Air conditioning in offices and homes compounds the problem by drawing transepidermal water out of an already barrier-compromised skin.
ECM skin booster is well-suited to this pattern because it addresses the matrix deficit that underlies all three problems at once. Restoring the structural lattice, it improves how the skin holds water, how it scatters light at the surface, and how it resists further breakdown. In my practice, the patient with the dry, dull, sun-damaged complexion that Singapore so reliably produces is one of the strongest indications for an ECM skin booster, and the clinical results in this group have been the most consistent of any indication I treat.
ECM skin booster is a powerful post-procedural and combination partner.
It rebuilds the foundation that lasers and energy devices treat at the surface.
Energy-based treatments such as fractional CO2, Pico laser, Thermage, Ultherapy, HIFU, Sygmalift, Infini RF microneedling, and Secret RF are extraordinary tools for surface resurfacing and dermal heating, but they work best on a substrate that has the underlying matrix to respond. A patient who undergoes a fractional laser session on a depleted ECM will see less of an improvement than the same patient on a well-supported matrix, because the regenerative response provoked by the laser depends on the cellular and matrix environment around it. This is the unspoken bottleneck in long-term aesthetic results in Singapore: the device is doing its job, but the substrate is not in a state to capitalise on it.
Combining ECM skin booster with energy-based treatments and complementary injectables is an emerging clinical pattern that I expect to become standard within the next two to three years. At The Clifford Clinic we time ECM skin booster sessions to either precede or follow specific energy device protocols depending on the indication. We also layer ECM skin booster with Profhilo or other hyaluronic acid boosters where hydration is a parallel concern. The product does not interfere with neuromodulators or with most laser modalities provided appropriate spacing. The one thing we do not combine ECM skin booster with in the same session is any procedure that disrupts the integrity of the freshly placed matrix, which excludes deep ablative resurfacing immediately after a Re2O injection.
ECM skin booster for men is a real indication, not a marketing afterthought.
Male skin has thicker dermis, slower turnover, and different ageing dynamics.
Male patient interest in regenerative skin treatments has grown sharply at The Clifford Clinic over the past two years, and ECM skin booster is one of the indications where the male anatomy actually justifies a slightly different protocol. Male skin tends to have a thicker dermis, denser sebaceous glands, and a different baseline ECM architecture from female skin. The visible signs of ageing tend to present later in life but progress faster once they begin, particularly in patients with significant outdoor activity, heavy alcohol use, or chronic sleep deprivation, which are common among the senior professionals I see in Raffles Place. Male patients also tend to want results that are not visually obvious as having been treated, which suits ECM skin booster’s natural and gradual profile.
The injection technique I use for male patients is broadly the same as for female patients, with two adjustments. I inject deeper to account for the thicker dermis, and I tend to use slightly larger aliquot volumes because the skin will tolerate them without surface irregularity. The endpoint patient experience is also a little different. Male patients tend to be more focused on functional outcomes, such as a less tired-looking face after a long week, rather than on glow or radiance metrics, and the ECM skin booster timeline of structural rather than cosmetic improvement aligns well with that priority.
What an ECM skin booster session at The Clifford Clinic actually looks like.
From numbing to needle to the realistic results timeline.
A patient arriving for an ECM skin booster session at our clinic should plan for an appointment of about ninety minutes from arrival to departure, although the actual injection time is far shorter than that. The first twenty to thirty minutes are devoted to a topical anaesthetic, applied across the full treatment area, which is most often the cheeks, lateral face, perioral zone, and, where indicated, the lower forehead and neck. While the anaesthetic takes effect, I reconstitute the freeze-dried ECM skin booster matrix at the bedside with sterile saline, in the proportions and timing specified in the L&C Bio protocol. In many cases, I also add a small volume of non-crosslinked hyaluronic acid to the reconstituted mix, both to improve flow through the injection needle and to layer in immediate surface hydration alongside the structural component.
The injection phase itself usually takes fifteen to twenty minutes. I place small aliquots of the reconstituted matrix across the mid-dermis at a depth of roughly 1.5 to 3 millimetres, adjusted to the local thickness of the skin in each zone, and I work in a grid pattern that ensures even dispersion. Most patients describe the sensation as a series of brief, tolerable pricks with intermittent pressure, far milder than what they have experienced with polynucleotide injections or with energy-based devices. Afterwards, I review aftercare with the patient, record the batch and lot numbers of the product used for the regulatory thirty-year traceability log, and walk them through the realistic results timeline.
That timeline is one of the most important things to set correctly at the first session, because ECM skin booster is the opposite of an immediate-glow treatment. Most patients notice the first faint improvements in skin texture and surface dewiness within the first week. The more noticeable changes in pore size and finer skin grain become visible between weeks four and eight as the fibroblast response gathers momentum. The structural firming and elasticity gains continue to build for three to six months after the third session in a typical course. Patients who arrive expecting a Profhilo-style four-week glow are often confused by the first month, until I remind them that they paid for matrix remodelling rather than hydration. By the third month, they understand.
How long ECM skin booster lasts, what side effects to expect, and what to do if something feels off.
A complete picture, not a sanitised marketing summary.
An initial course of ECM skin booster at The Clifford Clinic consists of three sessions spaced four to six weeks apart, followed by individualised maintenance every four to six months, depending on the patient’s age, skin condition, lifestyle factors, and the parallel treatments they are receiving. The structural improvements from a full initial course tend to persist for six to twelve months at peak, with a gradual decline thereafter as the body’s natural ECM turnover catches up. The maintenance interval is shorter for patients in their forties and fifties than for patients in their thirties, and shorter still in patients with heavy UV exposure, smokers, or those with chronic sleep deprivation.
In our clinical experience at the Clifford Clinic, the side effect profile is consistent with what Lee et al. reported in 2026. The common short-term effects include mild redness, swelling, and small palpable bumps at the injection sites in the first twenty-four to forty-eight hours. Occasional bruising can persist up to a week, more often in patients on aspirin, fish oil, or anti-inflammatory medications. Less common effects include persistent nodules that take longer than expected to resolve, mild tenderness, and transient asymmetry in patients with naturally different facial volumes. Serious complications such as infection, prolonged inflammatory reactions, or the rare vascular events associated with any midface injection are uncommon but real, and they are disclosed in detail during the informed consent process before any needle goes in.
The aftercare instructions are practical. Apply cool compresses for the first evening if swelling is noticeable. Avoid strenuous exercise, sauna, steam rooms, and aggressive heat for two to three days. Avoid alcohol and aspirin-containing medications for twenty-four hours. Use gentle, fragrance-free skincare for the first three days and reintroduce active ingredients such as retinoids only once all surface bumps have settled. Protect the treated zone with broad-spectrum sunscreen daily. If anything during recovery does not feel right, whether that is unusual asymmetry, severe pain, vision changes, or signs of infection such as warmth and spreading redness, contact The Clifford Clinic directly rather than waiting for the next scheduled appointment.
Injection technique, depth, and reconstitution matter more for ECM skin booster than for any other booster.
This is not a product to administer casually.
Hyaluronic acid boosters tolerate a wide range of injection techniques and still produce a reasonable result. ECM skin boosters do not. The clinical outcome of an ECM skin booster session depends heavily on three technique variables that most patients never see and that vary widely between clinics. The first is reconstitution. The ECM skin booster matrix is supplied as a freeze-dried powder that must be reconstituted at the bedside with sterile saline, in a defined volume, with a defined waiting period for full rehydration. Reconstituting too quickly, too thinly, or too late will reduce dispersion uniformity and lead to surface irregularity.
The second variable is injection depth. The matrix needs to land in the mid-dermis, which in most facial zones means a depth between 1.5 and 3 millimetres adjusted to skin thickness. Injection too superficial produces palpable surface bumps that resolve slowly. Injection too deep dilutes the structural effect because the matrix is no longer in the layer where fibroblast activity matters most. The third variable is aliquot size and dispersion pattern. The matrix needs to be distributed in small uniform aliquots across the treatment zone, not concentrated in a few large boluses. This is why the injection phase takes fifteen to twenty minutes for a full face rather than a few quick passes.
The implication for patients is unromantic but important. The ECM skin booster experience varies more between injectors than the patient might assume from looking at clinic marketing material. Asking your doctor how many cases of this product they have personally performed, which product brand they use, how they handle reconstitution, and what their personal injection depth and pattern preferences are is one of the more useful pre-treatment conversations to have.
The ten questions patients ask me most often (FAQ)
Direct answers to the questions that come up at almost every consultation.
| What is an ECM skin booster?
An ECM skin booster is an injectable treatment that delivers a micronised powder of human acellular dermal matrix into the mid-dermis. The matrix provides a physical scaffold of collagen, elastin, and other extracellular matrix proteins that the body integrates as its own tissue. It is different from a hydration booster (which adds water), a polynucleotide booster (which sends repair signals), and a collagen stimulator (which provokes the cells to make more collagen). How long doesECM skin booster last? After a full initial course of three sessions, the structural improvements tend to peak at three to six months and persist meaningfully for six to twelve months, with a gradual decline thereafter. Maintenance sessions every four to six months keep the matrix improvements at peak. Is ECM skin booster safe? The 2026 randomised controlled trial (Lee YI et al., International Journal of Molecular Sciences, PubMed 41828422) reported no serious adverse events. The product is manufactured by L&C Bio under American Association of Tissue Banks accreditation, with FDA tissue listing and Korean MFDS registration. Common side effects are mild and short-lived, primarily redness, swelling, and small bumps for one to two days. Does ECM skin booster hurt? Most patients describe the injection as tolerable. A topical anaesthetic is applied for twenty to thirty minutes before the procedure, which makes the actual injections feel like brief pinpricks with intermittent pressure. Patient reports place the discomfort meaningfully lower than polynucleotide injections like Rejuran. How is ECM skin booster different from Rejuran? Rejuran’s active ingredient is polynucleotide derived from salmon DNA, and it works by signalling the skin to repair. ECM skin booster’s active ingredient is micronised human acellular dermal matrix, and it works by physically supplying the matrix material the skin has lost. The two are best understood as complementary rather than competing, and many patients benefit from a layered plan that uses both. When will I see results from ECM skin booster? Some patients notice a subtle improvement in skin texture within the first week. More noticeable changes in pores and skin grain typically appear between weeks four and eight. The full structural firming continues to build for three to six months after the third session in a standard initial course. Can ECM skin booster be combined with lasers or HIFU? Yes, with appropriate spacing. ECM skin booster combines well with most laser and energy-based protocols when timing is planned to allow the matrix to settle before any procedure that would disrupt it. The product also layers cleanly with neuromodulators and with hyaluronic acid boosters in the same treatment plan. Who should not have ECM skin booster? Patients with active skin infection in the treatment zone, untreated inflammatory flare such as active cystic acne or uncontrolled rosacea, current pregnancy or lactation, current anticoagulant therapy without prior clearance from the prescribing physician, and any history of severe allergic reaction to injectable products should not have this treatment. A full clinical assessment is required before treatment in any patient. What is hADM actually made of? Human acellular dermal matrix is composed of approximately 89 percent Type I and Type III collagen, 7.6 percent other extracellular matrix proteins including fibronectin, laminin, tenascin and native growth factors, 3 percent elastin, and 0.4 percent glycosaminoglycans including hyaluronic acid. It is donor human dermal tissue that has been processed through a multi-step decellularisation protocol that removes all cells, DNA and lipids while preserving the native protein scaffold. How many ECM skin booster sessions do I need? The standard initial course at The Clifford Clinic is three sessions spaced four to six weeks apart. After the initial course, individualised maintenance sessions every four to six months keep the structural improvements at peak. The exact number for any patient depends on age, skin condition, parallel treatments, and clinical assessment at consultation. |
Why is ECM skin booster offered at The Clifford Clinic, and what to ask at your consultation.
The clinical philosophy behind a product is as important as the product itself.
ECM skin booster is offered at The Clifford Clinic for three reasons that have nothing to do with marketing and everything to do with how we think about regenerative dermatology in Singapore. The first reason is the mechanism. After more than a decade of administering hyaluronic acid boosters, polynucleotide injectables, and collagen stimulators, we have become increasingly aware of the ceiling those products hit in patients with significant structural decline. The matrix substrate is the bottleneck, and no amount of hydration or signalling solves a substrate problem. The arrival of an injectable that supplies the substrate directly closed a category gap that had been open for a long time.
The second reason is the evidence. The Lee et al. 2026 trial was the first large, properly blinded, head-to-head clinical study against a hyaluronic acid control that demonstrated meaningful superiority for an ECM-based booster across multiple objective skin parameters. Independent mechanistic work, including Liu and Sun’s JAK2 and STAT3 paper, anchored the molecular explanation. The L&C Bio manufacturing pedigree, with AATB accreditation, FDA listing, MFDS registration, and the long Korean track record, removed the regulatory and tissue-safety concerns that a less-substantiated hADM product would have raised. We would not have introduced this treatment without that evidence base in place.
The third reason is patient fit. Singapore is a market where the patient population has tried many injectables, has plateaued at the hydration level, and is increasingly aware that something more structural is needed. ECM skin booster is the appropriate product for that population. It does not replace Profhilo, Rejuran, or Sculptra. It complements them. It also adds something none of them could add, which is matrix material in the dermis.
| Dr Law Zhi Wei, Aesthetic Doctor
The most useful question a patient can ask at consultation is not whether ECM skin boosters work. The published trial settles that. The most useful question is whether ECM skin boosters are the right answer for this patient, in this skin condition, at this stage of their aesthetic plan. The answer is sometimes no. I have declined to treat patients whose primary concern is volume loss, where a filler is the right tool, or whose primary concern is hydration alone, where a Profhilo session would deliver the same satisfaction at lower cost and intervention. The strongest indication for Elravie ECM skin booster is the patient with visible structural decline, plateaued response to other boosters, and the patience to follow a three-session course over the better part of three months. For those patients, in my clinical experience at The Clifford Clinic over the past year, the clinical results have been the most consistent of any injectable I have introduced into my practice. Questions to bring to your consultation How many ECM skin booster treatments has the doctor personally performed? Which product brand is being used, and is the manufacturer’s traceability documentation available on request? How does the doctor decide between ECM skin booster, Rejuran, Profhilo, and a collagen stimulator for the specific concern the patient walks in with? What is the recommended initial course and maintenance schedule for this patient specifically? What is the doctor’s protocol if an unexpected nodule or prolonged swelling develops after a session? How is the regulatory thirty-year traceability for tissue-derived products maintained at this clinic? |
Further reading and the companion overview
If this guide has been more detail than you were looking for, Dr Gerard Ee’s shorter overview on The Clifford Clinic website is the natural companion piece (click here for the quick five-minute introduction to ECM skin boosters in Singapore). A series of focused companion articles covering each comparison and indication discussed above is in preparation and will be linked from this section as each one is published.
Booking a consultation at The Clifford Clinic
ECM skin booster is not the right treatment for every patient, and any responsible consultation should begin with a clinical assessment of whether it is the right treatment for you. If you have read this guide and your skin condition matches the indications described in section 12, the next step is a consultation with our team at The Clifford Clinic, 50 Raffles Place, #01-01 Singapore Land Tower, Singapore 048623, accessible directly from Exit B of Raffles Place MRT. We will review your skin condition, your treatment history, your parallel routine, and your aesthetic goals before any decision about ECM skin booster or any alternative is made. Appointments can be arranged on (65) 6532 2400 or WhatsApp (65) 8318 6332.
References
- Lee YI, Chau NH, Nguyen NH, Ham S, Baek Y, Kim J, Lee JH. Injectable Particulated Human Acellular Dermal Matrix Booster for Skin Restoration: An Integrated Randomized, Split-Face, Double-Blinded Clinical Trial and Preclinical Study. International Journal of Molecular Sciences, 2026. PubMed: 41828422. PubMed Central: PMC12985180. DOI: 10.3390/ijms27052193.
- Liu C, Sun J. A porcine acellular dermal matrix induces human fibroblasts to secrete hyaluronic acid by activating JAK2 and STAT3 signalling. RSC Advances, 2020. PubMed: 35518338.
- Yue D, Wu X, Song H, Zhou Z, Ye M, Zhu M. The Application of the Acellular Dermal Matrix in the Correction of the Tear Trough Deformity. Aesthetic Plastic Surgery, 2018. PubMed: 30097671.
- Fisher GJ, Varani J, Voorhees JJ. Looking older: fibroblast collapse and therapeutic implications. Archives of Dermatology, 2008.
- Shin JW, Kwon SH, Choi JY, Na JI, Huh CH, Choi HR, Park KC. Molecular Mechanisms of Dermal Aging and Antiaging Approaches. International Journal of Molecular Sciences, 2019.
- Yi KH, Winayanuwattikun W, Kim SY, et al. Skin boosters: Definitions and varied classifications. Skin Research and Technology, 2024.
- Ghatge AS, Ghatge SB. The Effectiveness of Injectable Hyaluronic Acid in the Improvement of the Facial Skin Quality: A Systematic Review. Clinical, Cosmetic and Investigational Dermatology, 2023.
- Kirsner RS, Bohn G, Driver VR, et al. Human acellular dermal wound matrix: evidence and experience. International Wound Journal, 2015.
- Petrie K, Cox CT, Becker BC, MacKay BJ. Clinical applications of acellular dermal matrices: A review. Scars, Burns and Healing, 2022.
- L&C Bio. Elravie Re2O product specifications (on file). Composition, AlloClean Technology, regulatory accreditation summary. 2024 to 2026.
- ClinicalTrials.gov. Safety and Efficacy of an ECM-Based Intradermal Injectable for Skin Rejuvenation. NCT07155278.
- Singapore Statutes Online. Healthcare Services (Advertisement) Regulations 2021 under the Healthcare Services Act 2020.
- Singapore Medical Council. Guidelines on Aesthetic Practices for Doctors.
- Health Sciences Authority Singapore. Cell, Tissue and Gene Therapy Products (CTGTP) regulatory framework.
- American Association of Tissue Banks (AATB). Standards for Tissue Banking. Donor screening, tissue recovery, and processing standards.