



Knee Pain And Stiffness? How Platelet-Rich Plasma Injections Utilises Orthobiologics To Combat Knee Osteoarthritis And Promote Cartilage Repair
Platelet-rich plasma (PRP) therapy is an emerging non-surgical first line treatment for knee pain that is often used together with other treatments like hyaluronic acid (HA) knee joint injections. Knee Osteoarthritis (OA) is a characterised by reduced mobility accompanied by aching pain, stiffness, and swelling of the knee joint. And as mentioned, it can be treated with PRP injections. But what is PRP?
In this blog post we will discuss the causes of knee osteoarthritis, what is PRP, what makes intraarticular PRP knee injections standout from other OA treatments and the benefits of knee filler + PRP combination therapy.
What is knee osteoarthritis?
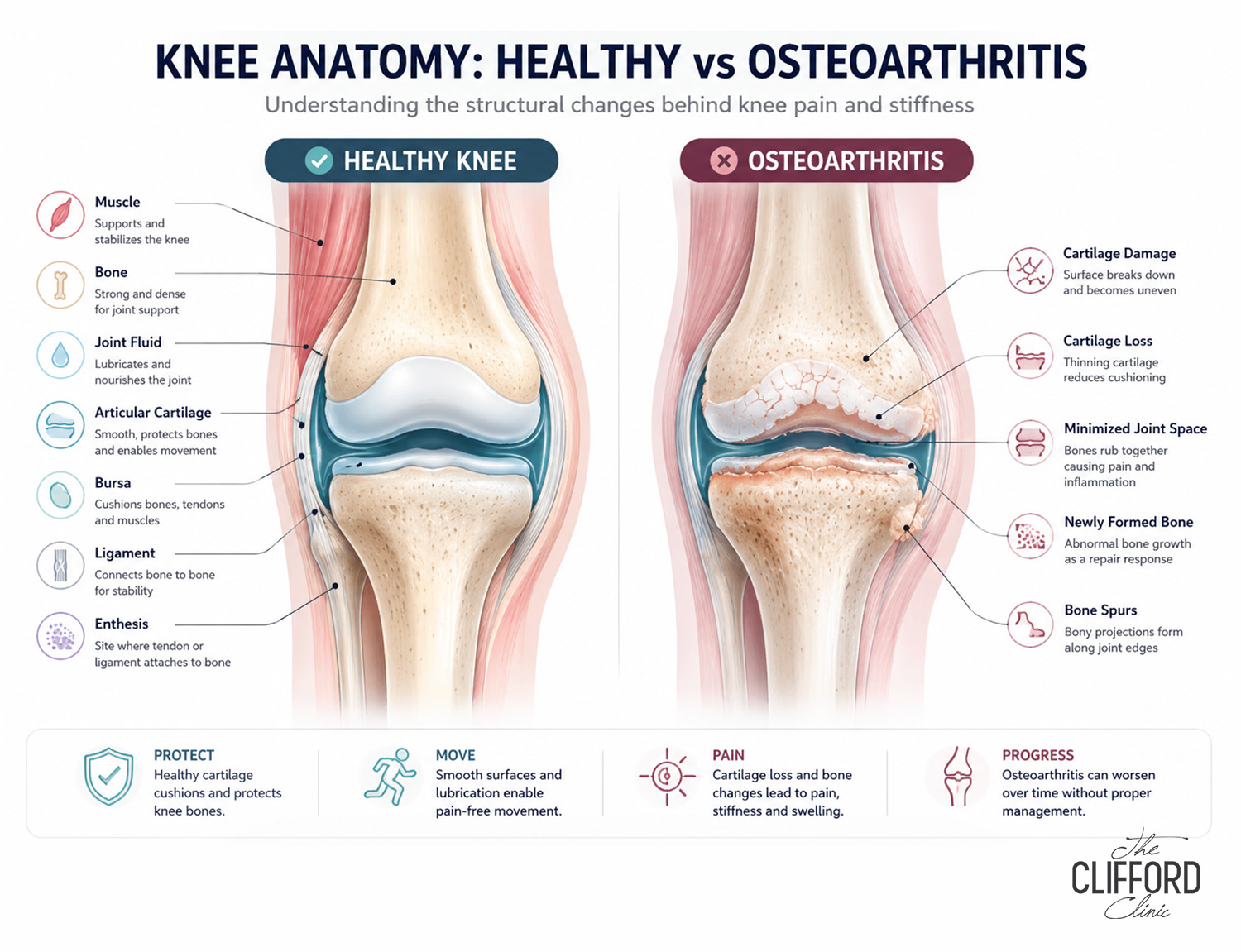
The medical term “osteoarthritis” is derived from the Greek words for bone (osteo-), joint (arthr-) and inflammation (-itis). However, while the word “inflammation” is in its name, inflammation is actually not the primary cause of osteoarthritis. Rather, osteoarthritis is caused by the breakdown of cartilage in the joints and underlying bone.
Knee osteoarthritis is a progressive and multifactorial degenerative joint disease, specifically affecting the knee joints that is caused by the gradual wearing away of cartilage in the joint (articular destruction). Knee OA is also characterised by a decrease in both the quality and concentration of synovial fluid (naturally occurring knee joint lubricant).
Symptoms include:
- Knee pain – knee OA is characterised by a persistent dull uncomfortable ache or sharp pain that is exacerbated by even mild physical activity like walking, squatting, or climbing the stairs.
- Stiffness – the affected knee(s) may feel stuck or locked up when you attempt to move it, especially after sitting or not moving the knee for an extended period of time.
- Inflammation/swelling – the affected knee may appear visibly swollen and/or feel boggy to the touch. In some cases, the knee joint may also feel warm when touched.
- Reduced mobility/functional impairment – pain and stiffness can make it difficult to bend or straighten the knee joint affecting mobility. For some, the knee may also feel like it will buckle or collapse when used, causing instability and further difficulty walking. In cases where the pain becomes debilitating, the patient may even become unable to walk.
- Crepitus – crepitus is described as a popping/clicking/grinding/creaking noise or sensation felt when the knee is moved.
What causes cartilage breakdown?
Articular cartilage is a smooth and glass-like specialised type of hyaline cartilage composed of type II collagen and proteoglycans that covers the ends of bones in synovial joints (such as the knees), it acts as both a shock absorber and enabler of low-friction joint movement.
Cartilage naturally breaks down as you age due to mechanical wear and tear, however, genetics (e.g. weak leg muscles or structural instability caused by misaligned joints), joint trauma (e.g. torn ligaments or bone damage), excessive mechanical stress (e.g. heavy lifting due to a job/sport or chronic obesity) and constant repetitive joint stress (e.g. high-impact sports like running, or frequent kneeling due to a job) can accelerate cartilage degradation.
Is knee osteoarthritis curable or reversible?
Damage to knee joint cartilage is considered irreversible due to the inability of adult articular cartilage to naturally regenerate/grow back on its own once worn down.
As damage to the cartilage is not easily or naturally reversible, most conventional treatment options for knee OA aim to manage pain, slow down the deterioration of the remaining knee cartilage, or surgically replace/realign the knee joint to restore function instead of “undoing” or “repairing” the damage. The exception to this is Platelet-Rich Plasma (PRP) injections/PRP therapy, owing to this particular treatment’s ability to stimulate natural repair while reducing inflammation.
The Clifford Clinic’s multipronged approach to OA management
Generally, knee OA is more effectively managed when treated by a combination of different treatment types. For example, knee joint injections can be used in tandem with a compression sleeve (an assistive device) and weight management. While all of the following treatments can be used on their own to treat mild to moderate OA, we recommend a “mix and match” approach for better results:
- Platelet-Rich Plasma (PRP) injections – PRP therapy utilises the patient’s own platelets to stimulate cartilage tissue repair and regeneration. As a single brief paragraph is insufficient to explain the scope of PRP therapy, please read the dedicated sections on PRP therapy below for the full picture.
- Knee joint injections – also known as viscosupplementation. During this treatment, hyaluronic acid (HA) is injected into the knee joint for the purpose of replacing depleted synovial fluid to achieve pain relief, restore joint lubrication, and improve the quality and concentration of synovial fluid.
- Corticosteroid injections – corticosteroids are fast-acting anti-inflammatory drugs that reduce joint swelling and provide instant relief. While not permanent, effects of steroid injections can last for a few weeks up to a few months.
- Weight management – excess weight can put extra strain on the knee joints, speeding up wear and tear. Weight management through exercise, nutrition therapy/a nutritional diet plan, or the use of semaglutides (prescription weight loss medication) can slow down joint degradation.
- Assistive devices – the affected knee can be supported via the use of compression sleeves, braces, or walking canes to improve mobility and reduce discomfort/pain.
- Physical therapy – physical therapy can help patients regain mobility by improving joint flexibility and strengthening leg muscles.
- Pain medication – oral or topical pain relievers can be used to manage chronic pain and provide short term relief.
For more severe cases of knee OA, surgery can be considered:
Knee arthroplasty (knee replacement surgery) – a surgical procedure that replaces damaged bone, joint surfaces, and/or cartilage with artificial implants. Partial Knee Replacement or Total Knee Replacement can be performed depending on the severity of the joint damage. - Osteotomy – a surgical procedure that adjusts the alignment, angle, or length of the tibia (shin bone) and/or femur (thigh bone) via cutting or removing sections of said bone. Osteotomy can relieve pain and improve knee stability and function by realigning the knee joint or shifting weight away from damaged cartilage.
- Knee arthroscopy (key-hole surgery) – minimally invasive surgical procedure where a specialised tube camera (an arthroscope) and small surgical tools are inserted into the knee/joint via small incisions that are made around the knee. As only a few small cuts (keyholes) are needed for diagnosis and damage repair, key-hole surgery is less painful and has a faster recovery time compared to knee arthroplasty or osteotomy.
What is platelet-rich plasma (PRP) therapy?
Platelet-rich plasma therapy is a non-surgical autologous regenerative treatment that uses your own blood platelets to reduce inflammation and promote joint tissue healing and regeneration by injecting PRP that is “harvested” from your own blood into the treatment area/damaged tissue.
PRP vs blood
Platelet-Rich Plasma is not the same as regular unprocessed blood, meaning we are not just drawing blood from your arm and reinjecting it back into your knee. Blood is composed of red blood cells, white blood cells, and platelets (thrombocytes) suspended in plasma, while, as the name suggests, the two main components of PRP are:
- Platelets (thrombocytes) – fragments of cytoplasm produced by megakaryocytes (large bone marrow cells) located in bone marrow or lung tissue. Platelets play a major role in the body’s blood clotting mechanism, but more importantly (in relation to OA treatment), platelets contain bioactive proteins like cytokines and growth factors which promote wound healing and regeneration.
- Plasma – liquid component of blood that makes up around 55% of your body’s total blood volume. It is the suspension medium for the platelets and their cytokines and growth factors.
How is PRP made?
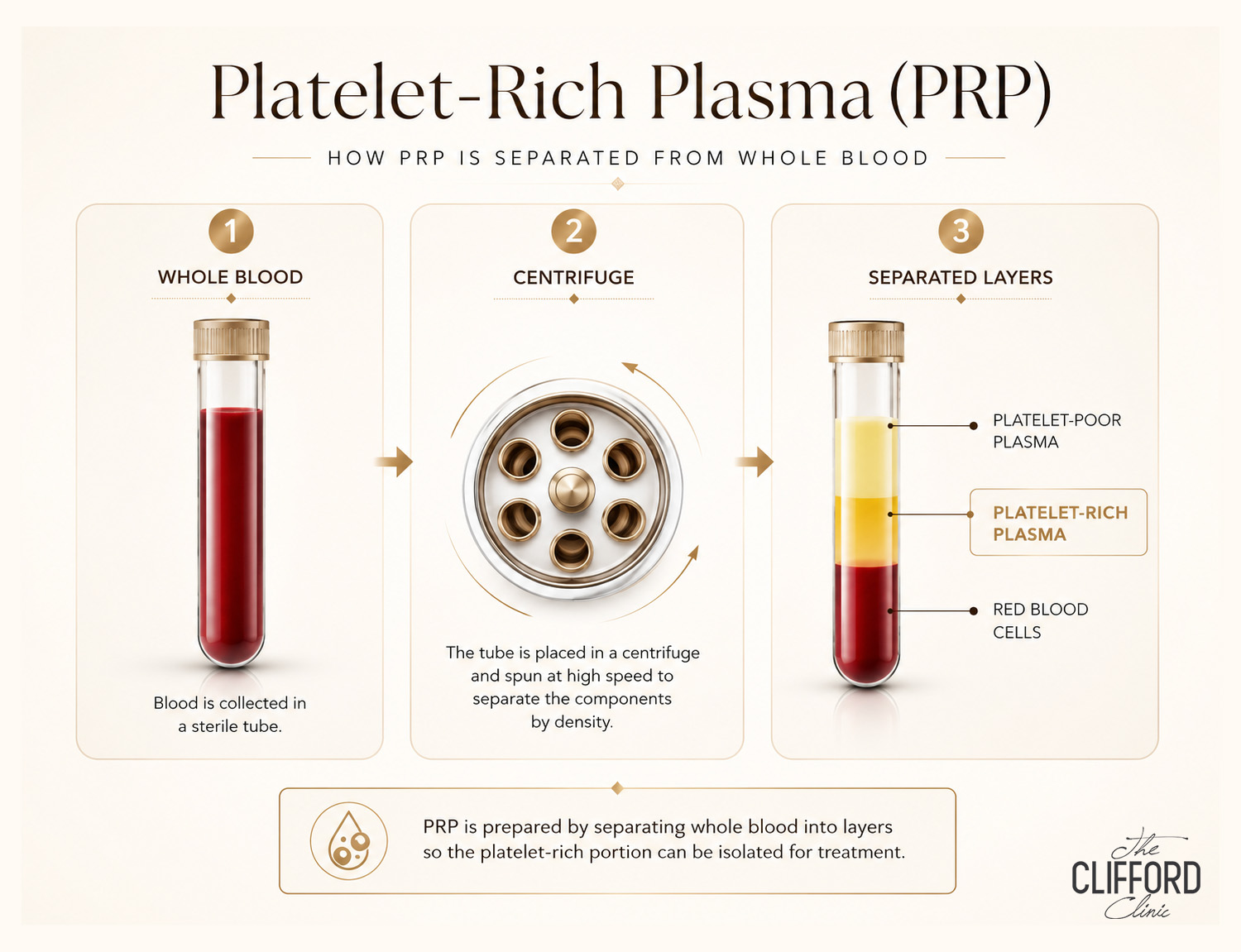
Once the blood sample is collected from your arm, the sample is placed into a centrifuge for the first “soft” spin to separate your blood into three distinct layers based on their density: the top plasma layer, the middle “buffy coat” layer that contains the platelets and white blood cells, and the bottom red blood cell layer.
The red blood cell layer is removed and the plasma and buffy coat layers are then spun for a second time (the “hard” spin) to concentrate just the platelets at the bottom of the sample tube. This concentrated layer of platelets is the PRP that is used for the injection.
Benefits of PRP therapy
The high concentration of growth factors in PRP stimulates cellular activity in the tissue of the injection site, allowing PRP therapy to not just manage the symptoms of OA and slow down its progression, but also repair joint damage. In short, the main benefits of PRP therapy are:
- Ability to reduce inflammation and alleviate pain.
- Promotion of natural tissue healing and cell regeneration.
- Promotion of collagen production; Collagen is needed to maintain the structural framework and tensile strength of cartilage.
- Non-allergenic and does not trigger an immune response as it is an autologous therapy.
- Cartilage regeneration via Platelet-Rich Plasma injections
- PRP therapy stands out from other OA treatments owing to its ability to reverse existing tissue damage.
Adult Knee articular cartilage is unable to/possesses very limited ability to regenerate naturally on its own as it lacks blood vessels, nerves, and a lymphatic system; A direct blood supply is needed for the delivery of component and cells that are needed for tissue repair, thus, articular cartilage is unable to jumpstart the healing response on its own due to its avascular (lack of blood supply) nature.
PRP injections circumvent the limited regenerative capacity of articular cartilage by directly delivering a high concentration of your own growth factors to the damaged cartilage to kickstart the natural repair process.

Growth factors that can be found in PRP that are vital for cartilage repair:
- Platelet-Derived Growth Factor (PDGF) – stimulant for chondrocyte (collogen producing cell) proliferation and survival. PDGF works in tandem with hyaluronic acid in the synovial fluid to restore and maintain the structural integrity and resilience of knee cartilage.
- Vascular Endothelial Growth Factor (VEGF) – a signalling protein that promotes angiogenesis (new blood vessel formation) and militance of existing blood vessels.
- Insulin-like Growth Factor-1 (IGF-1) – stimulates the production of molecules that are essential for cartilage structural integrity by chondrocytes and supresses the breakdown of cartilage matrix.
- Transforming Growth Factor-β (TGF-β) – the TGF-β superfamily of signalling proteins are key components in the regulation of cell proliferation and differentiation, they are needed for the specialisation and maturity (differentiation) of chondrocytes and for the synthesis of cartilage matrix.
Effectiveness of Platelet-Rich Plasma injections for pain relief
Corticosteroid injections are the most well-known treatment for OA-associated pain. However, a recent medical study published in the Journal of Orthopaedic Surgery comparing the effectiveness of intra-articular (inside a joint) PRP injections versus corticosteroid injections for the treatment of knee OA and found that PRP injections produced superior long-term pain management outcomes.
A group of patients presenting with a history of chronic pain and reduced knee joint mobility due OA (presence of OA was verified via X-ray imaging) where split into two groups: one group was given PRP injections, while the other group was given corticosteroid injections.
The study found that while corticosteroids produced better initial results (faster pain relief upon injection), the effects of corticosteroids only lasted around 15 weeks post-injection, with reports of the initial pain returning or steadily increasing after the 15-week period.
In contrast, the effects of PRP injections lasted up to 30 weeks post-treatment; Patients who received PRP therapy reported sustained pain relief during the 30-week period and a slower return/increase of the initial pain after the 30-week period.
Effectiveness of PRP therapy for restoring knee function
With reference to the same study mentioned in the section above, PRP therapy was shown to be effective in both managing OA symptoms and restoring knee function. This study measured knee function using International Knee Documentation Committee (IKDC) and Knee Society Score (KSS).
Knee function improvement was seen in both the group that was given PRP injections and the group that was given corticosteroid injections up to 5 to 15 weeks post-treatment. However, the group that received PRP injections continued to show significant improvement in IKDC and KSS scores compared to the group that received corticosteroids up till one year post treatment.
In summary, PRP therapy was shown to outperform corticosteroids:
- PRP injections have a longer duration of action – the therapeutic effects of PRP lasting up to 30 weeks (some studies report effectiveness up to 12 months) as compared to corticosteroids that lose effectiveness at around 15 weeks post injection.
- PRP therapy repairs damage and restores function – corticosteroids pain relief but are unable to undo existing cartilage damage or stimulate tissue healing and cartilage repair like PRP therapy.
- PRP therapy produces better long-term patient outcomes – corticosteroids are superior for short-term immediate pain relief, but studies show that while PRP therapy takes 15 to 30 weeks to deliver their best results, PRP therapy provides greater pain relief in the long term in addition to improving knee function.
The Clifford Clinic’s recommendation for knee OA treatment
We recommend PRP therapy with knee fillers for a more well-rounded OA treatment plan – while PRP therapy produces superior patient outcomes, we recognise that it is a treatment that works best in the mid to long-term; PRP therapy lacks the ability of treatments like corticosteroid injections or knee fillers to provide immediate/short-term relief and protection from further damage.
Synergy of knee fillers with PRP injections
Synovial fluid is the body’s natural joint lubricant, it is composed of mainly hyaluronic acid (HA, also known as hyaluronan), lubricin, proteins, and water. Knee OA causes degradation of the synovial membrane and thus a decrease in the quantity and/or quality of synovial fluid produced, leading to increased joint friction. This negative feedback loop is one of the driving factors knee OA progression.
When used together with PRP injections, patients are able to reap the longer lasting long-term regenerative and anti-inflammatory benefits of PRP therapy while enjoying the faster acting benefits of knee fillers:
- Almost immediate pain relief – pain relief is expected within one-week post-injection.
- Fast lubrication – Knee fillers are made from HA or its derivative, hylan. When injected into the knee, they mimic natural synovial fluid and act as an immediate replacement for the decrease in the quantity of synovial fluid present.
- Shock absorption – inflammation due to OA can cause an increase the total volume of synovial fluid in the joint due to leaky blood vessels. This volume increase dilutes the existing HA that is in the synovial fluid, leading to loss of viscoelasticity due to decrease in HA concentration. Knee fillers immediately increase viscoelasticity by bolstering HA concentration.
Complications associated with untreated osteoarthritis
If left untreated, knee OA can lead to joint instability as the muscles that support the joint become weaker due to disuse; It is not uncommon for those suffering from knee OA to avoid exercise or adopt a more sedentary lifestyle due the pain felt when moving their knee joint.
In more severe cases, knee OA can lead to further complication such as the development of bone spurs when the loss of cartilage causes increased friction on the joint, leading to the development of unnatural extra growths of bone tissue on the bones of the knee joint (the extra growths appear as lumps or “spurs” on the bone). These spurs can cause irritation to soft tissue surrounding the joint and further hinder joint mobility.
A popliteal cyst, also known as a Baker’s cyst, can form when excess synovial fluid is produced in reaction to cartilage breakdown due to OA. Synovial fluid is usually produced in a small amount as a lubricant for the knee joint. However, when cartilage is damaged, the joint may compensate for the damage by producing extra fluid to cushion itself. Pooling of the excess fluid in the knee joint can result in a fluid-filled lump forming behind the knee, this lump is the Baker’s cyst. If left untreated it can burst and cause bruising and sharp pain to the calf and knee, and vein thrombosis in rare cases.
Whilst most well known for his expertise in dermatology and aesthetic procedures, Dr Gerard Ee (Medical Director of The Clifford Clinic and Surgery) is also an expert in knee pain management and orthopaedic care.
As a correct diagnosis is the first step to receiving appropriate treatment/care, Dr Ee would like to alert our readers on the possibility of meniscal cysts masquerading as Baker’s cysts. There are two types of cysts that can develop as a result of injury to the knee joint:
- Baker’s cysts (popliteal cysts) – fluid-filled sacs caused by the pooling of excess synovial fluid in the popliteal space at the back of the knee.
- Meniscal cysts – fluid-filled sac caused by synovial fluid escaping via a tear in the meniscus cartilage.
In most cases, swelling or bulging at the back of the knee joint is indicative of a Baker’s cyst as meniscal cysts usually form next to the tear in meniscus cartilage, meaning they tend to form on the side of the knee instead of at the back of the knee joint.
However, as per his medical paper published in The Open Orthopaedics Journal (an international, peer-reviewed medical journal), Dr Ee cautions that while rare, a horizontal tear in the medial meniscus can result in a meniscal cyst that presents as a large bulge or swelling at the back of the knee that closely mimics a Baker’s cyst; such a cyst is known as a central voluminous postero-medial meniscal cyst.
Quoting his paper, ‘Not Always a Baker’s Cyst’ – An Unusual Presentation of a Central Voluminous Postero-Medial Meniscal Cyst, a patient was originally misdiagnosed by a general practitioner with having a Baker’s cyst due to the location of the swelling. As Baker’s cysts are often treated more conservatively using mild measures like rest, compression, applying ice, or physical therapy, while larger meniscal cysts may require needle aspiration or surgery to correct the meniscus tear, the misdiagnosis led to the patient suffering from recurrent pain over the course of a year.
Dr Ee notes that thankfully in this case, the misdiagnosis was corrected after an MRI scan of the knee was performed. MRIs are vital for differentiating between the two types of cysts as the MRI scan will reveal the meniscus tear.
If you are ever unsure if you have a Baker’s cyst or a meniscal cyst, or if you have been diagnosed with having a Baker’s cyst but find that you are unresponsive to treatment, we recommend getting a second opinion from a medical practitioner who specialises in knee pain, such as Dr Ee, as soon as possible as this is a condition where an incorrect diagnosis can greatly impact your quality of life.