


Clinical Research, Publications and Medical Insights by Clifford Clinic
Publications
Management of the neglected and healed bilateral cervical facet dislocation
Date: 2014
Doctor Author: Gerard Ee, Abhishek Srivastava, Chan Wearn Benedict Peng, Seang Beng Tan, , Benjamin Phak Boon Tow
Research type- Grand Rounds article / case report
Treatment area- Orthopaedics; spine surgery; cervical spine trauma and reconstructive management of neglected bilateral cervical facet dislocation
Publication Summary
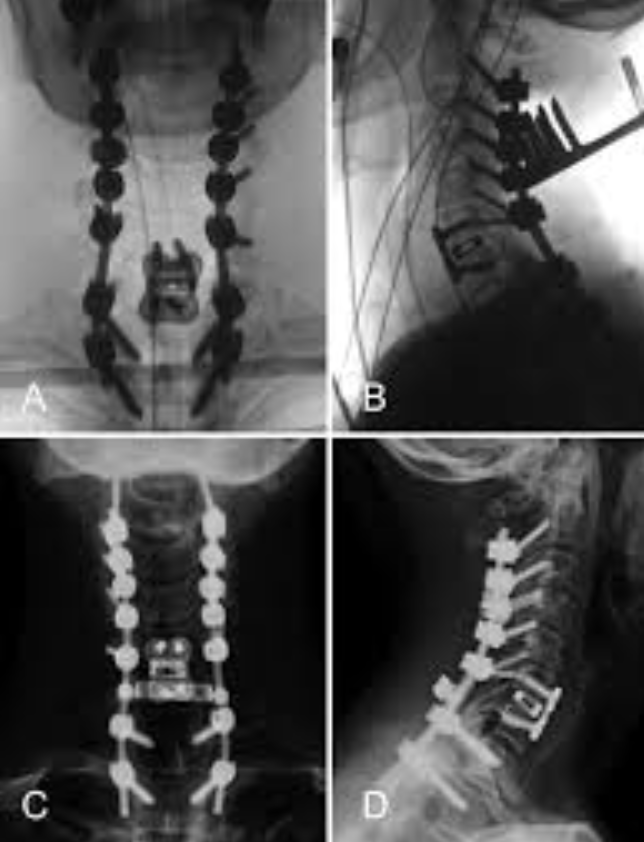
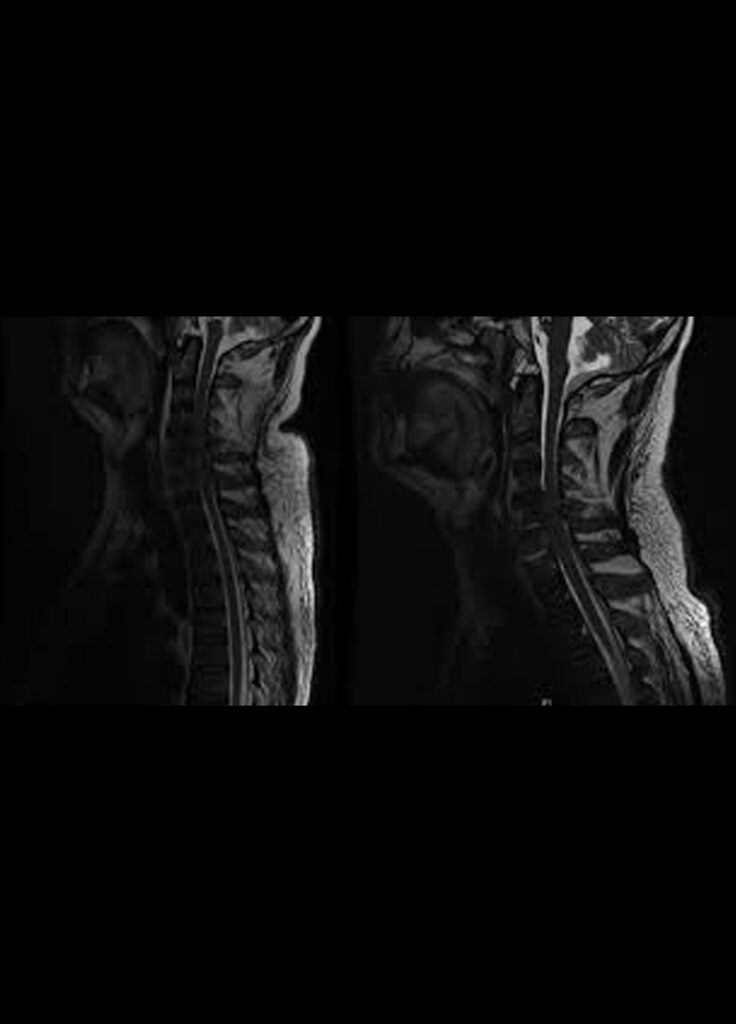
Case report: A 42-year-old male was pushed into a 1.2-m pool by accident and hit his head on the bottom. He immediately felt a sharp pain in his neck but was able to get out of the pool by himself and at the emergency department was found to have no neurological deficit. Standard trauma radiographs were performed and a grade 1 anterolisthesis of C4 on C5 was observed without any facet subluxation or dislocation. An emergent Magnetic Resonance Imaging (MRI) of the cervical spine confirmed X-ray results and in addition demonstrated injury to the posterior ligament complex and a broad-based posterior disc bulge. Computed Tomography (CT) scans revealed no facet dislocation or fractures. Unfortunately, the patient failed to come for his follow-up visits and at 14 months post injury, represented with pain and deformity with impairment of horizontal gaze. Computed tomography and MRI demonstrated a fused (bony) bilateral facet dislocation at C4/5. A cervical spine reconstruction consisting of a posterior-anterior-posterior approach was performed to address both the deformity and the pain. At 32-month follow-up, the patient remains well with no neurological symptoms, minimal neck pain and successful fusion.
Conclusion: Current literature does not offer a clear solution to the management of healed neglected bilateral cervical facet dislocation. The presence of circumferential bony fusion around the deformity necessitates a posterior and anterior release and subsequent stabilization to address this complex problem. We also wish to highlight the order of the reconstructive approach and the need to recognize instability of the cervical spine despite
Clin Orthop Relat Res. 2014 Jun;472(6):1718-24. doi: 10.1007/s11999-013-3158-5. Epub 2013 Jul 12.
Date: 2013
Doctor Author: Gerard Ee, Lau Wen Liang, Yeo William, Von Bing Yap, Yue Wai Mun
Research type– Case-control study / retrospective comparative clinical study
Treatment area– Orthopaedics; spine surgery; minimally invasive spinal surgery, open spinal surgery and surgical site infection risk
Publication Summary
Methods: Medical records of 2299 patients who underwent transforaminal lumbar interbody fusion, laminectomy, or discectomy were analyzed and selected for a nested case-control analysis. Twenty-seven cases with SSI were matched with 162 control subjects without SSI stratified based on procedure performed within 28 days of the case’s date of surgery. Patients were identified from an institutional database at a tertiary care hospital. MIS involved spinal procedures performed through a tubular retractor system. Univariate and multivariate analyses were performed.
Results: Patients undergoing open spinal surgery were 5.77 times more likely to develop SSI compared with MIS approaches (odds ratio [OR], 5.77; 95% confidence interval [CI], 1.0-32.7; p = 0.048). Also, from the multivariate regression model, diabetes (OR, 4.7; 95% CI, 1.3-17.0; p = 0.018), number of levels operated on (OR, 3.5; 95% CI, 1.6-7.5; p = 0.001), and body mass index (OR, 1.2; 95% CI, 1.0-1.3; p = 0.010) were predictive of an increased risk in SSI. Staphylococcus aureus was most frequently identified, being present in 12 of 21 (52.4%) patients in whom positive cultures were obtained. Four of the 12 patients had methicillin-resistant S aureus infection.
Journal of Spinal Disorders and Techniques
J Spinal Disord Tech. 2015 Jul;28(6):E328-35. doi: 10.1097/BSD.0b013e31828f940c.
Date: 2013
Doctor Author: Gerard Ee, Lei Jiang, Chang Ming Guo, William Yeo, Seang Beng Tan, Benjamin Tow, John Chen, Wai Mun Yue
Research type: Comparative study / retrospective analysis of prospectively collected clinical data
Treatment area: Orthopaedics; spine surgery; osteoporotic vertebral compression fractures and vertebral augmentation outcomes
Publication Summary
Methods: The outcome measures were assessed for 6 months for those treated conservatively and up till 2 years for those treated surgically. Radiographic measurements of the spine were correlated with the clinical outcomes.
Results: A total of 62 patients (12.1%) were treated conservatively, 148 (40.8%) with vertebroplasty, 97 (26.7%) with balloon kyphoplasty, and 56 (15.4%) with sky bone expander. We found significant improvements in Visual Analog Score, Oswestry Disability Index, and Short-Form-36 scores for all groups after 1-month follow-up (P<0.05), with the surgical groups demonstrating a greater improvement in pain scores after the first postoperative day (P<0.0001) when compared with the conservative group. The improvements in outcomes in those treated surgically were sustained for up to 2 years with no significant difference (P>0.05) among the surgical groups. We also found significant improvement (P<0.005) in anterior vertebral and kyphotic wedge angle after surgical intervention.
A silent acute abdomen in a patient with spinal cord injury
British Medical Journal
BMJ Case Rep. 2013 Mar 27;2013:bcr2013008548. doi: 10.1136/bcr-2013-008548.
Date: 2013
Doctor Author: Gerard Ee, Pang SY, Kumar N, Malhotra R
Research type: Case report
Treatment area: Orthopaedics; spinal cord injury; acute abdomen and abdominal perforation in patients with impaired neurological sensation
Publication Summary
Abstract: A 52-year-old man with cervical spondylosis sustained a hyperextension injury to the neck and subsequently developed central cord syndrome after 2 weeks. The diagnosis was confirmed clinically and on MRI. During the admission he was febrile from Streptococcus anginosus bacteraemia from a gum infection and was started on penicillin. This resulted in pseudomembranous colitis with abdominal distension and bloody diarrhoea but a lack of expected abdominal complaints. Unfortunately his neurology deteriorated and a repeat MRI showed a discitis at C5-C7 which required a 2-level discectomy, debridement and instrumented fusion. Owing to his spinal cord injury, an abdominal perforation was initially missed owing to the lack of clinical features of an acute abdomen. He underwent a right hemi-colectomy for ascending colon perforation and eventually made a good recovery and was discharged to a spinal rehabi
Evolution of arthroscopic shoulder stabilization: do we still need open techniques?
OA Orthopaedics. 2013 May 01;1(1):1-6. doi: 10.13172/2052-9627-1-1-527.
Date: 2013
Doctor Author: Gerard Ee, Andrew H, Sedeek S
Research type: Review article / critical literature review
Treatment area: Orthopaedics; shoulder surgery; arthroscopic shoulder stabilisation and open surgical techniques for recurrent anterior shoulder instability
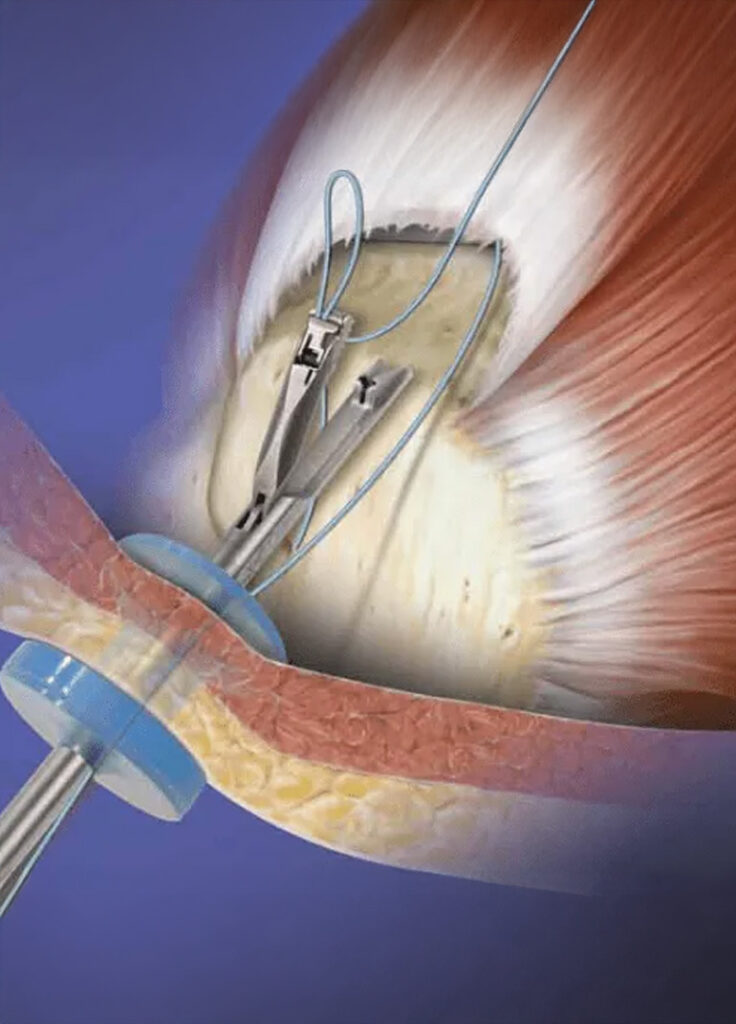
Publication Summary
Abstract: Recent studies show comparable results of arthroscopic shoulder stabilization techniques compared with the gold standard open Bankart reconstruction. Great technical advances and ever-increasing surgeon experience have rendered pathology once deemed an indication for open surgery as treatable by arthroscopic means. With this movement toward a more universal application of all-arthroscopic techniques, we might consider the following question: Is there ever a need to open? To answer this question, we must first consider normal anatomy and then appreciate the contribution of deranged pathoanatomy to recurrent instability in each individual case. The surgeon must then determine whether this is best addressed via an arthroscopic or open technique. Arthroscopy, as compared with open stabilization procedures, holds the potential benefits of decreased morbidity rates, early functional rehabilitation, and improved range of motion. Despite potential advantages, arthroscopic stabilization is clearly contraindicated when a significant pathologic lesion contributing to recurrent instability cannot be adequately addressed as a result of the limitations of current techniques or instrumentation. On the basis of this principle, we believe that sizable glenohumeral bone defects remain the only absolute contraindication to an all-arthroscopic approach. Many complicating issues, such as attenuated capsule, humeral avulsion of the glenohumeral ligament lesions, cases of revision surgery, and collision or contact athletes, exist and warrant close attention. We prefer to think of these situations as “challenges” for which both arthroscopic and open surgery should be considered, rather than as true contraindications to arthroscopic shoulder stabilization. We are, by no means, advocating arthroscopic treatment in all cases of shoulder instability, because this would represent a gross oversimplification of the issues at hand. However, we do acknowledge that the steadfast contraindications to arthroscopic shoulder stabilization are decreasing every day.

A subtrochanteric femoral fracture 15 years after radiotherapy: a case report
The Journal of Orthopaedic Surgery
J Orthop Surg (Hong Kong). 2013 Aug;21(2):253-7. doi: 10.1177/230949901302100229.
Date: 2013
Doctor Author: Gerard Ee, Harish Sivasubramanian, Manjunatha Ganiga Srinivasaiah, Shamal Das De
Research type: Case report
Treatment area: Orthopaedics; trauma surgery; radiation-associated pathological fracture and subtrochanteric femoral fracture management
Publication Summary
Abstract: Pathological fracture is a rare but serious complication of radiotherapy. We report on a 44-year-old man who presented with a subtrochanteric femoral fracture 15 years after radiotherapy for a soft-tissue sarcoma in the thigh. We discuss its potential causes, a scoring system to identify high-risk patients for prophylactic intramedullary nailing of the femur, and radiographic signs to identify an impending insufficiency fracture.
The Knee
Knee. 2013 Aug;20(4):256-262. doi: 10.1016/j.knee.2012.10.026. Epub 2012 Dec 7.
Date: 2012
Doctor Author: Gerard Ee, Hee Nee Pang, Hwei Chi Chong, Mann Hong Tan, Ngai Nung Lo, Seng Jin Yeo
Research type: Prognostic study / prospective clinical outcomes study
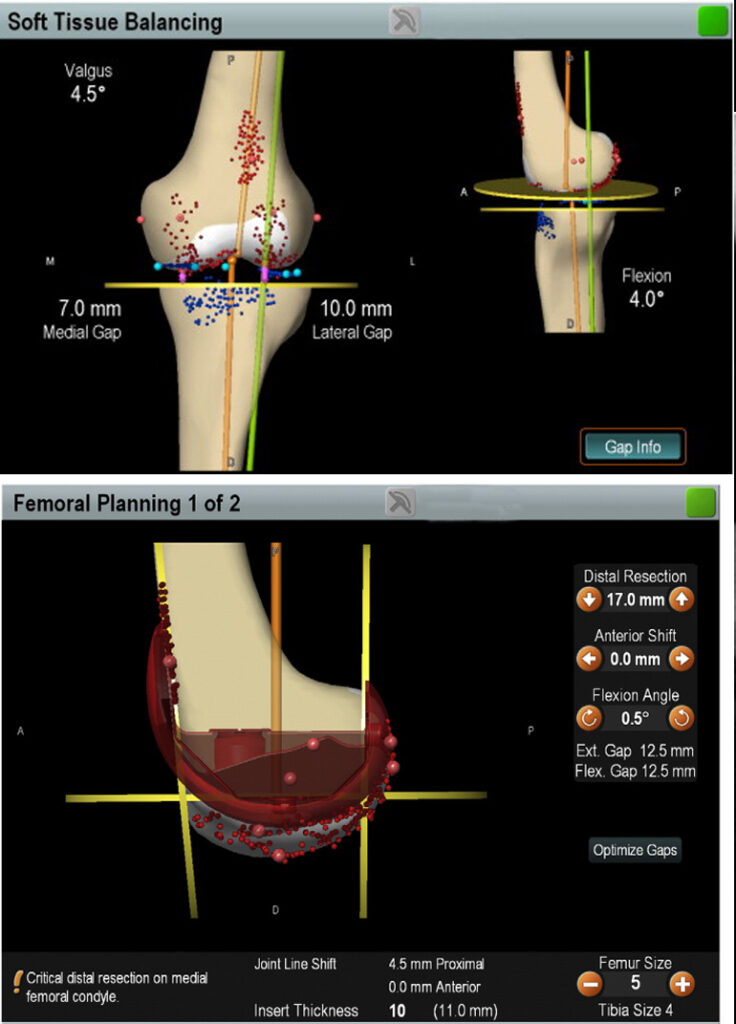
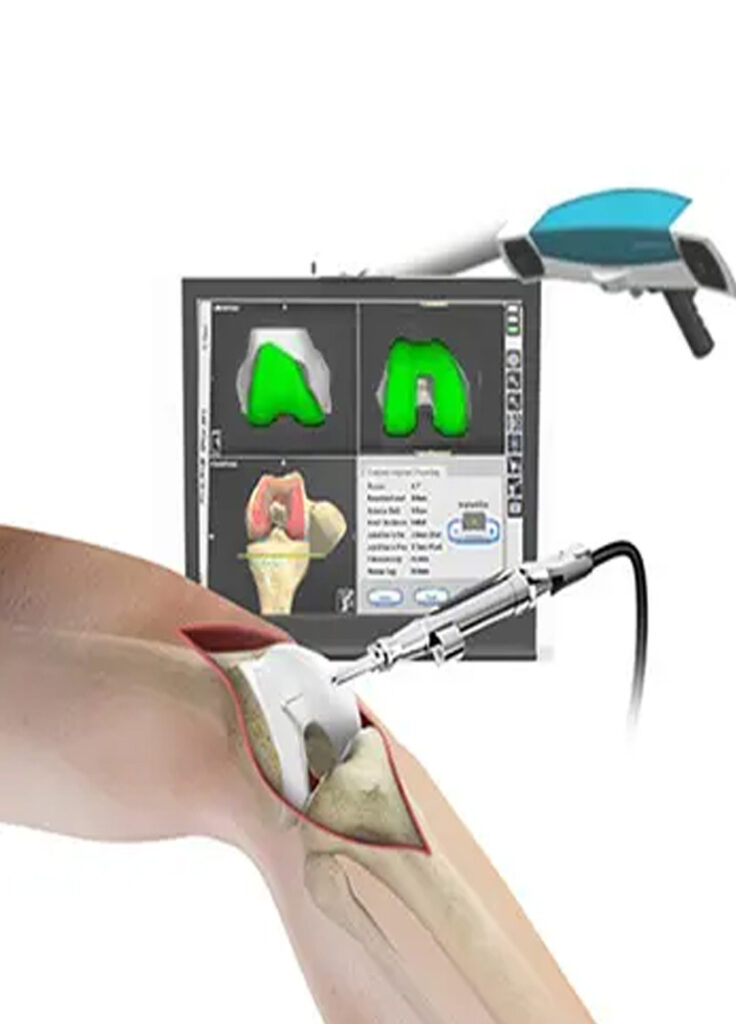
Treatment area: Orthopaedics; knee surgery; computer-assisted total knee arthroplasty and intra-operative joint line measurement
Publication Summary
Methods: One hundred sixty-eight patients (168 knees) underwent CAS TKA by two surgeons at a single institution with 2 years follow-up. The final change in joint line was calculated from the verified tibial resection and distal femoral cuts. Group A patients had joint line changes of less than 4mm and Group B patients had joint line changes of more than 4mm. Post-operative Oxford scores, Knee scores, Function scores and SF-36 scores were obtained at 6 months and 2 years post TKA.
Results: There was significant linear correlation between joint line changes and Oxford scores (P=0.0001), Function scores (P=0.0001) and Knee scores (P=0.0001) at 6 months and Oxford scores (P=0.0001) alone at 2 years with increasing joint line changes having poorer outcome scores. Group A compared to Group B patients demonstrated better Oxford scores (P=0.0001), Function scores (P=0.0001), Knee scores (P=0.0001) and total SF-36 scores (P=0.003) at 6 months as well as better Oxford scores (P=0.0001) and Knee scores (P=0.014) at 2 years.
The Open Orthopaedics Journal
Open Orthop J. 2012;6:424-8. doi: 10.2174/1874325001206010424. Epub 2012 Sep 20.
Date: 2012
Doctor Author: Gerard Ee, Harish Sivasubramanian, Manjunatha Ganiga Srinivasaiah, Shamal Das De, Sing AM
Research type: Case report
Treatment area: Orthopaedics; knee surgery; meniscal cysts and differential diagnosis of posterior knee swelling
Publication Summary
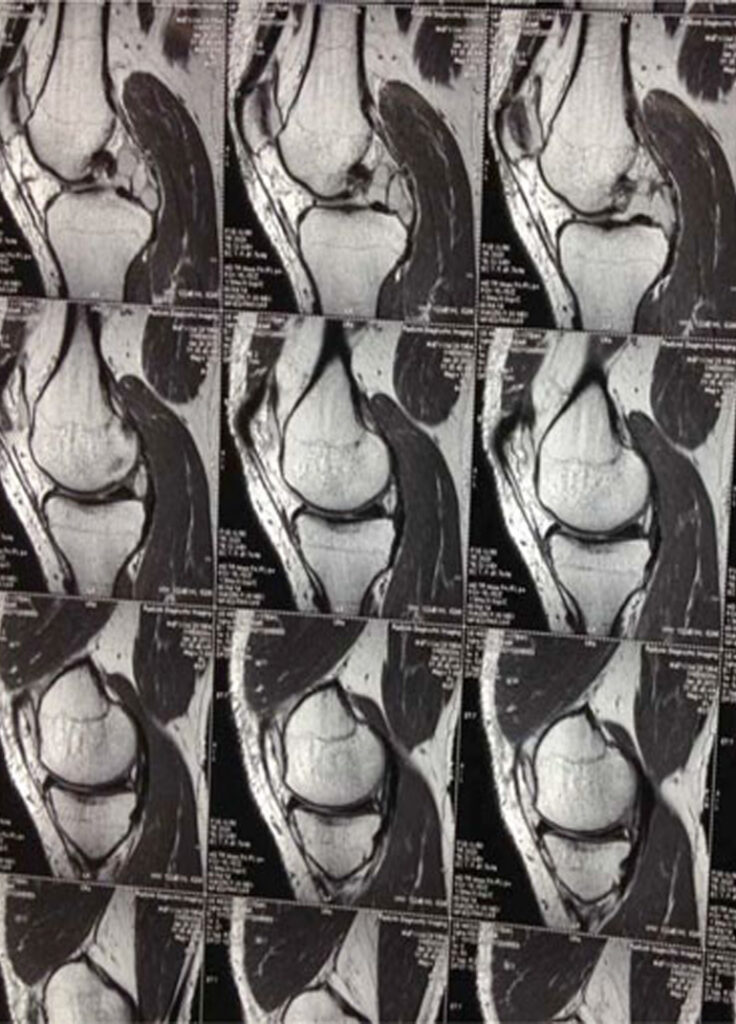
Abstract: Meniscal cysts are rare and often are a result of extrusion of synovial fluid through a tear of the meniscus, resulting in a one-way valve effect of the tear. Arthroscopic partial meniscectomy of the meniscus with intra-articular cyst drainage has become the standard of care. We report a case of an unusually large symptomatic medial meniscal cyst, situated postero-medially and pressing on the posterior cruciate ligament, which was initially clinically misdiagnosed as a Baker’s cyst. The patient had difficulty and pain on squatting. He was successfully treated with arthroscopic debridement and needle decompression; a rarity in literature for such a voluminous perilabral cyst tenting the posterior cruciate ligament. This procedure has the advantage of being able to obtain the cystic fluid for histological and cytological analysis before debridement. This case also highlights the importance of the use of Magnetic Resonance Imaging (MRI) to accurately diagnose a central, posterior knee swelling.

The Use of Gabapentin to Decrease Morphine Consumption After Surgical Debridement for Burns
Archives of Trauma Research
Arch Trauma Res. 2012 Summer;1(2):83-84. doi: 10.5812/atr.6468. Epub 2012 Aug 21.
Date: 2012
Doctor Author: Gerard Ee, Rachel Ho
Research type: Commentary / short academic article
Treatment area: Burns care; postoperative pain management; gabapentin use after surgical debridement of burn wounds
Publication Summary
Methods: In this article they recruited 50 patients and through a randomized, double-blind, placebo-controlled study demonstrated a significant improvement in pain scores and clinical parameters after administration of a single oral dose of 1200mg gabapentin.
Results: Despite no significant difference was demonstrated between the gabapentin group and the placebo group, I note that there was a decrease in respiratory rate at all-time points in the gabapentin group. I understand the rational of using these parameters as a mean in recording pain but would one not expect the increased use of opiates in the placebo group to result in a greater influence on respiratory depression? It would be worth commenting on this. Lastly, the authors have focused on the analgesic effect of gabapentin in burn patients. However, it would worth to mention the effect of gabapentin on post-burn pruritus as well. Post-burn pruritus has a reported incidence of between 80-100% and gabapentin has been proposed to have a modulating effect on this distressing symptom.

American Medical Journal
American Medical Journal. 2012;3(2):220-227. doi: 10.3844/amjsp.2012.220.227.
Date: 2011
Doctor Author: Wen Wei Gerard Ee, Wen Liang Joel Lau, Harish Sivasubramanian, Diarmuid Murphy
Research type: Review article / literature review
Treatment area: Orthopaedics; fracture healing; parathyroid hormone analogues and teriparatide use in human fracture repair
Publication Summary
Approach: We conducted a systematic review of multiple databases analysing papers within the last 10 years. All studies involving the use of PTH analogues in humans were included. All animal studies were excluded. Appropriate statistics regarding patient’s age, gender, site of fracture, teriparatide treatment regime, clinical outcomes and imaging outcomes were extracted, analysed and summarized.
Results: A total of 10 observational studies and 2 randomized controlled trials were evaluated in this study. With administration of teriparatide (PTH1-34), the mean time to 100% disappearance of fracture site pain was 3.1 months ±0.7 months. Delayed or non-union fractures achieved bony bridging in 4.3 months. For new fractures treated non-surgically, there have been reports of shorter time to cortical bridging in the treatment group (7.4 weeks, n = 34, p = 0.006) as compared to the control group (9.1 weeks, n = 34). Lastly, a total of 8 out of 254 patients (3.1%) experienced mild side effect from teriparatide administration.

Long term results of arthroscopic Bankart repair for traumatic anterior shoulder instability
Journal of Orthopaedic Surgery and Research
J Orthop Surg Res. 2011 Jun 14;6:28. doi: 10.1186/1749-799X-6-28.
Date: 2011
Doctor Author: Gerard WW Ee, Sedeek Mohamed, Andrew HC Tan
Research type: Research article / clinical outcomes case series
Treatment area: Orthopaedics; shoulder surgery; arthroscopic Bankart repair for traumatic anterior shoulder instability
Publication Summary
Methods: Data from 79 shoulders in 74 patients were collected over 4 years (2004 – 2008). Each patient was followed-up over a period of 2 years. The patients underwent arthroscopic Bankart repair using bio-absorbable suture anchors for their shoulder instability. These surgeries were performed at a single institution by a single surgeon over the time period. The patients were assessed with two different outcome measurement tools. The University of California at Los Angeles (UCLA) shoulder rating scale and the Simple Shoulder Test (SST) score. The scores were calculated before surgery and at the 2-year follow-up. The recurrence rates, range of motion as well post-operative function and return to sporting activities were evaluated.
Results: SST results from the 12 domains showed a significant improvement from a mean of 6.1 ± 3.1 to 11.1 ± 1.8 taken at the 2-year follow-up (p < 0.0001). Data from the UCLA scale showed a Pre and Post Operative Mean of 20.2 ± 5.0 and 32.4 ± 4.6 respectively (p < 0.0001). 34 had excellent post-operative scores, 35 had good scores, 1 had fair score and 3 had poor scores. 75% of the patients returned to sports while 7.6% developed a recurrence of shoulder dislocation or subluxation.
Computer navigation improves accuracy of Joint Line restoration in Total Knee Arthroplasty
Journal of Bone and Joint Surgery British
J Bone Joint Surg Br. 2012;94-B(SUPP XLIV):30.
Date: 2011
Doctor Author: Gerard Ee, Hee Nee Pang, Hwei Chi Chong, Shi Lu Chia, Pak Lin Chin, Ngai Nung Lo, Mann Hong Tan, Seng Jin Yeo
Research type: Conference abstract / clinical orthopaedic study
Treatment area: Orthopaedics; knee surgery; computer-assisted total knee arthroplasty and joint line restoration
Publication Summary
Methods: One hundred sixty-eight patients (168 knees) underwent CAS TKA by two surgeons at a single institution with 2 years follow-up. The final change in joint line was calculated from the verified tibial resection and distal femoral cuts. Group A patients had joint line changes of less than 4mm and Group B patients had joint line changes of more than 4mm. Post-operative Oxford scores, Knee scores, Function scores and SF-36 scores were obtained at 6 months and 2 years post TKA.
Results: There was significant linear correlation between joint line changes and Oxford scores (P=0.0001), Function scores (P=0.0001) and Knee scores (P=0.0001) at 6 months and Oxford scores (P=0.0001) alone at 2 years with increasing joint line changes having poorer outcome scores. Group A compared to Group B patients demonstrated better Oxford scores (P=0.0001), Function scores (P=0.0001), Knee scores (P=0.0001) and total SF-36 scores (P=0.003) at 6 months as well as better Oxford scores (P=0.0001) and Knee scores (P=0.014) at 2 years.

Minimally invasive Unicondylar Knee Arthroplasty in a Patellectomized Patient
Knee Surgery, Sports, Traumatology, Arthroscopy
Knee Surg Sports Traumatol Arthrosc. 2012 Sep;20(9):1831-1833. doi: 10.1007/s00167-011-1787-3.
Date: 2011
Doctor Author: Gerard Ee, Hee Nee Pang, Ngai-Nung Lo, Seng Jin Yeo
Research type: Case report
Treatment area: Orthopaedics; knee surgery; minimally invasive unicondylar knee arthroplasty in a patellectomized patient
Publication Summary
Abstract: Patellectomized patients may have less satisfactory clinical outcomes following total knee arthroplasty due to a decreased extensor mechanism efficiency and potential instability. The literature only reports 3 case series of patients who had a previous patellectomy undergoing a Unicondylar Knee Arthroplasty (UKA) with mixed results. A Minimally Invasive fixed-bearing UKA was performed in a patellectomized patient with excellent postoperative knee stability and clinical outcomes after 5 years. MIS UKA may be a viable option for patellectomized patients with isolated medial compartment osteoarthritis and no preoperative extensor deficiency or instability.
The patellofemoral syndrome; the same problem as the Loch Ness Monster?
The Knee
Knee. 2009 Oct;16(5):301-302. doi: 10.1016/j.knee.2009.05.005. Epub 2009 Jul 18.
Date: 2009
Doctor Author: Gerard Ee, Ronald Grelsamer, Garrett Moss, Simon Donell
Research type: Editorial / clinical commentary
Treatment area: Orthopaedics; knee surgery; patellofemoral pain syndrome, anterior knee pain and diagnostic terminology
Publication Summary
Abstract: The patellofemoral syndrome does not exist, and studies that have purported to investigate it are as tantalising, but ultimately as fruitless as the shadowy pictures of the monster in Loch Ness. We would suggest that the term “anterior knee pain” describes the problem without implying a diagnosis or a physical condition, and is the only symptom that we can all actually agree on.
Date: Dec 2013
Doctor Author: Goh YS, Law ZW, Tiong HY
Journal of Urology, 2013 Dec;190(6):2309–10.
Research type- Peer-reviewed correspondence / academic commentary
Treatment area- Urology; prostate biopsy infection prevention
Publication Summary
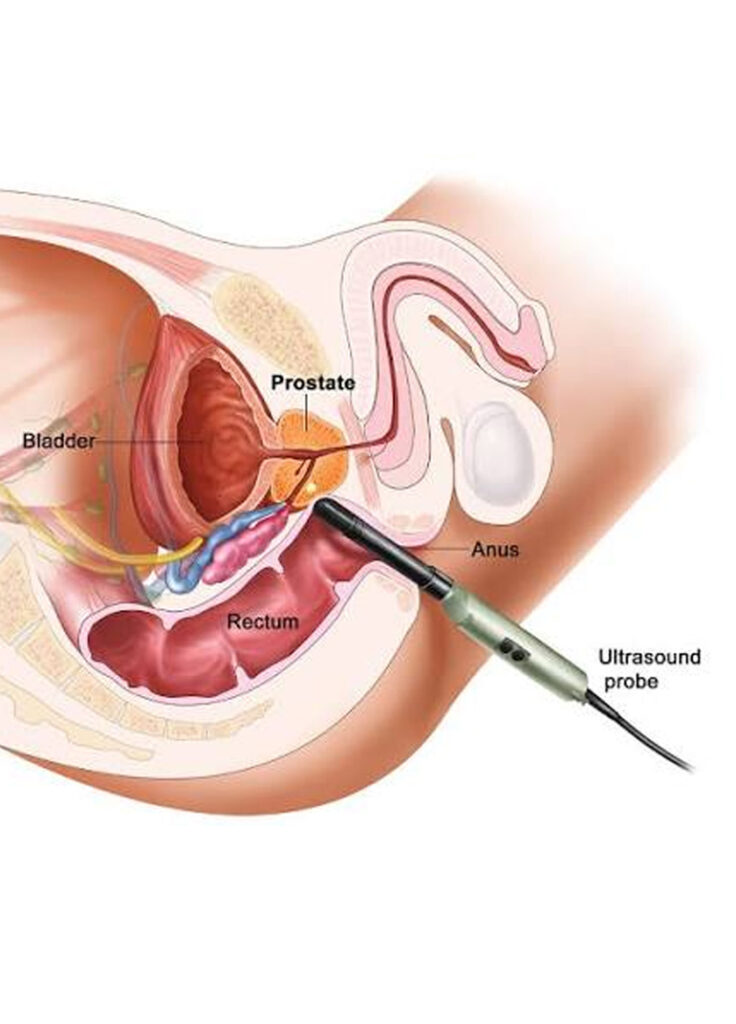
Materials and methods: Between 2009 and 2011, 865 men were prospectively randomized to rectal cleansing (421) or no cleansing (444) before transrectal ultrasound guided prostate biopsy. Patients received ciprofloxacin prophylaxis and rectal swab cultures were obtained before transrectal ultrasound guided prostate biopsy. Patients completed a telephone interview 7 days after undergoing the biopsy. The primary end point was the rate of infectious complications, a composite end point of 1 or more of 1) fever greater than 38.0C, 2) urinary tract infection or 3) sepsis (standardized definition). Chi-square significance testing was performed for differences between groups and a multivariate analysis was performed to assess risk factors for infectious complications.
Results: Infectious complications were observed in 31 (3.5%) patients, including 11 (2.6%) treated and 20 (4.5%) control patients (p = 0.15). Sepsis was observed in 4 (1.0%) treated and 7 (1.6%) control patients (p = 0.55). On multivariate analysis resistance to ciprofloxacin in the rectal swab culture (p = 0.002) and a history of taking ciprofloxacin in the 3 months preceding transrectal ultrasound guided prostate biopsy (p = 0.009) predicted infectious complications.
Date: 2020
Doctor Author: Lim KS, Law ZW, Chow MWL, Sim ASP, Ho HSS
Asian Journal of Urology, 2020 Oct;7(4):357–362.
Research type- Pilot prospective randomised single-blinded trial
Treatment area- Urology; ureteral stent discomfort and post-stent pain management
Publication Summary
Methods: Forty adults requiring retrograde unilateral ureteral stent placements were enrolled. Patients with single ureteric stone or benign stricture were selected. Patients were randomised in 1:1 ratio to the loop and pigtail arm. The USSQ was administered before placement (baseline), USSQ and VAS were administered on Day 3, 7, and 14.
Results: There were no significant differences between the USSQ scores. Median pain scores on Day 3 were lower in the loop stent group (2.9 vs. 4.0, p=0.047). There was a significant reduction in pain from Day 3–7 (0 vs. −1, p=0.016) in the pigtail group.
Date: Sept 2018
Doctor Author: Law ZW, Chen K, Neo SH, Yuen SPJ, Sim SPA
European Urology Supplements, 2018;17(7):e2439.
Research type- Pilot clinical study / conference abstract
Treatment area- Urology; robotic-assisted radical prostatectomy and postoperative catheter management
Publication Summary
Methods: Forty adults requiring retrograde unilateral ureteral stent placements were enrolled. Patients with single ureteric stone or benign stricture were selected. Patients were randomised in 1:1 ratio to the loop and pigtail arm. The USSQ was administered before placement (baseline), USSQ and VAS were administered on Day 3, 7, and 14.
Results: There were no significant differences between the USSQ scores. Median pain scores on Day 3 were lower in the loop stent group (2.9 vs. 4.0, p=0.047). There was a significant reduction in pain from Day 3–7 (0 vs. −1, p=0.016) in the pigtail group.
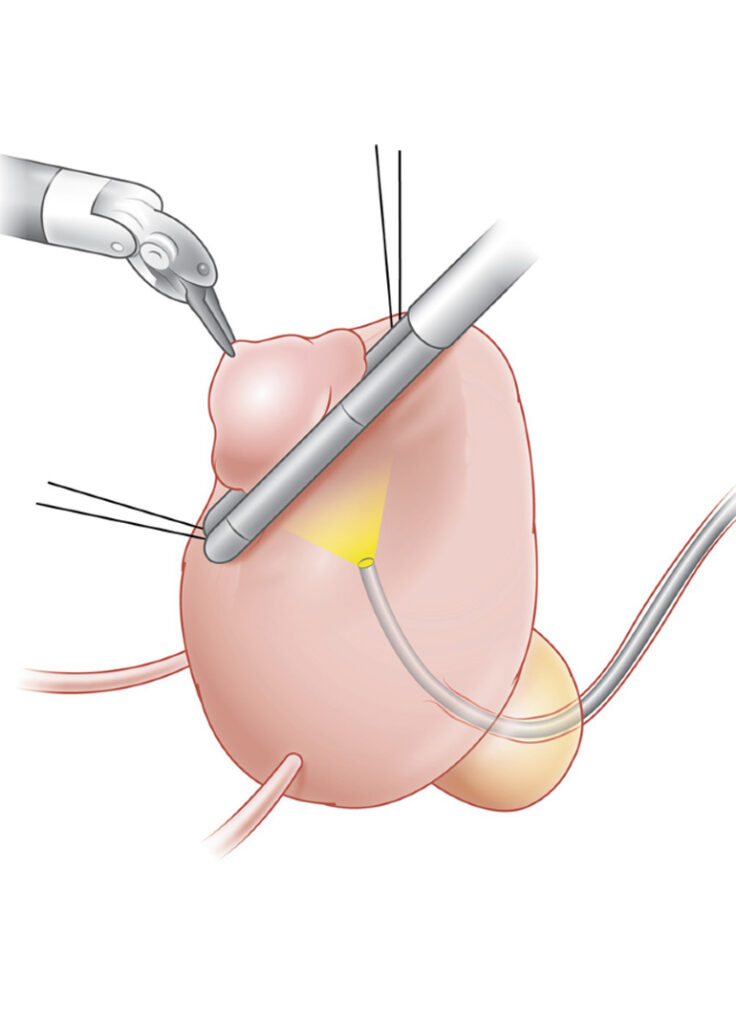
Robotic-Assisted Laparoscopic Partial Cystectomies (RAPC) for Urachal Diseases — The Ideal Choice
Date: 2018
Doctor Author: Yong J, Law ZW, Chen K, Sim SPA, Lee LS, Yuen SPJ
European Urology Supplements, 2018;17(7):e2451.
Research type- Conference abstract / surgical technique and case series
Treatment area- Urology; robotic-assisted partial cystectomy for urachal diseases
Publication Summary
Methods: Two men and two women with a mean age of 51.5±9.3 years underwent RLPC between June 2009 and December 2009. In each case, a single surgeon using the da Vinci-S robotic system (Intuitive Surgical, Sunnyvale, CA, USA) used a transperitoneal approach with a 0° robotic camera. After careful observation of the intravesical portion of the mass, the mass was excised by use of monopolar scissors circumferentially. The bladder was closed in two layers with watertight running sutures made with 2-0 Vicryl.
Results: The mean operative time was 198 minutes (range, 130-260 minutes), the mean console time was 111 minutes (range, 70-150 minutes), and the mean estimated blood loss was 155 ml. The urethral catheter was removed on postoperative day 7 after a normal cystogram, and the surgical drain was removed on postoperative day 2.5 (range, 2-3 days). The mean hospital stay was 6 days (range, 4-7 days). There were no major complications. The pathology report revealed that one patient had a urachal cystadenoma, two patients had a urachal cyst, and one patient had a patent urachus.
Date: Sept 2020
Doctor Author: Yong J, Law ZW, Yang XY, Ng TK, Yuen JS
Urology Video Journal, 2020 Sep;7:100039.
Research type- Surgical video article / small case series
Treatment area- Urology; robotic-assisted partial cystectomy for urachal diseases
Publication Summary
Methods: A systematic review was conducted using PubMed, Scopus, the Cochrane Library, and ScienceDirect (last search: 1 November 2024). Inclusion criteria encompassed studies reporting on RAUEPC for urachal pathologies, while non-robotic approaches and incomplete data were excluded. Risk of bias was assessed using the Newcastle-Ottawa Scale for cohort studies and the JBI Critical Appraisal Checklist for Case Reports. Descriptive statistics summarized continuous data (means, medians, 95% confidence intervals), and chi-square tests analyzed associations between categorical variables. Heterogeneity analysis was infeasible, necessitating narrative synthesis. Institutional retrospective data from three cases (2021–2024) were included for comparison. This study was registered in PROSPERO (CRD42024597785). No external funding was received.
Results: A total of 44 studies (n = 145) met the inclusion criteria. Benign lesions accounted for 66.2% and malignant lesions for 33.8%. Mean operative time was 177.8 min (cumulative), 162.7 min (benign), 192.2 min (malignant), 85.33 min (institutional, 95% CI: 74.13–96.53). Mean blood loss was 85.4 mL (cumulative), 99.5 mL (benign), 72.7 mL (malignant), 216.66 mL (institutional). Mean hospital stay was 3.64 days (cumulative), 3.26 days (benign), 4.36 days (malignant), 6.33 days (institutional, 95% CI: 3.46–9.20). Complications occurred in 10.04% (cumulative), 11.82% (benign), 8.57% (malignant), with one minor event (Clavien–Dindo II) in institutional cases. No conversions to open surgery were reported. All cases achieved complete excision with no R1 resections. No recurrences were observed at 10.66-month (institutional) mean follow-up.
Date: 2020
Doctor Author: Law ZW, Ho H, Yuen SPJ, Teo J, Huang HH, Cheng WS
Presented at Urofair 2013, AUA 2013, and SIU 2013.
Research type- Single-centre prospective clinical experience / conference abstract
Treatment area- Urology; robotic-assisted transperineal prostate biopsy and prostate cancer diagnosis
Publication Summary
Methods: A systematic review was conducted using PubMed, Scopus, the Cochrane Library, and ScienceDirect (last search: 1 November 2024). Inclusion criteria encompassed studies reporting on RAUEPC for urachal pathologies, while non-robotic approaches and incomplete data were excluded. Risk of bias was assessed using the Newcastle-Ottawa Scale for cohort studies and the JBI Critical Appraisal Checklist for Case Reports. Descriptive statistics summarized continuous data (means, medians, 95% confidence intervals), and chi-square tests analyzed associations between categorical variables. Heterogeneity analysis was infeasible, necessitating narrative synthesis. Institutional retrospective data from three cases (2021–2024) were included for comparison. This study was registered in PROSPERO (CRD42024597785). No external funding was received.
Results: A total of 44 studies (n = 145) met the inclusion criteria. Benign lesions accounted for 66.2% and malignant lesions for 33.8%. Mean operative time was 177.8 min (cumulative), 162.7 min (benign), 192.2 min (malignant), 85.33 min (institutional, 95% CI: 74.13–96.53). Mean blood loss was 85.4 mL (cumulative), 99.5 mL (benign), 72.7 mL (malignant), 216.66 mL (institutional). Mean hospital stay was 3.64 days (cumulative), 3.26 days (benign), 4.36 days (malignant), 6.33 days (institutional, 95% CI: 3.46–9.20). Complications occurred in 10.04% (cumulative), 11.82% (benign), 8.57% (malignant), with one minor event (Clavien–Dindo II) in institutional cases. No conversions to open surgery were reported. All cases achieved complete excision with no R1 resections. No recurrences were observed at 10.66-month (institutional) mean follow-up.
Robotic-Assisted Laparoscopic Partial Cystectomies (RAPC) for Urachal Diseases — The Ideal Choice
Date: 2018
Doctor Author: Law ZW, Yong J, Chen K, Sim SPA, Lee LS, Yuen SPJ
BJU International, Sep 2018 (Supplement). Presented at ERUS Marseilles 2018.
Research type- Conference abstract / surgical technique and case series
Treatment area- Urology; robotic-assisted partial cystectomy for urachal diseases
Publication Summary
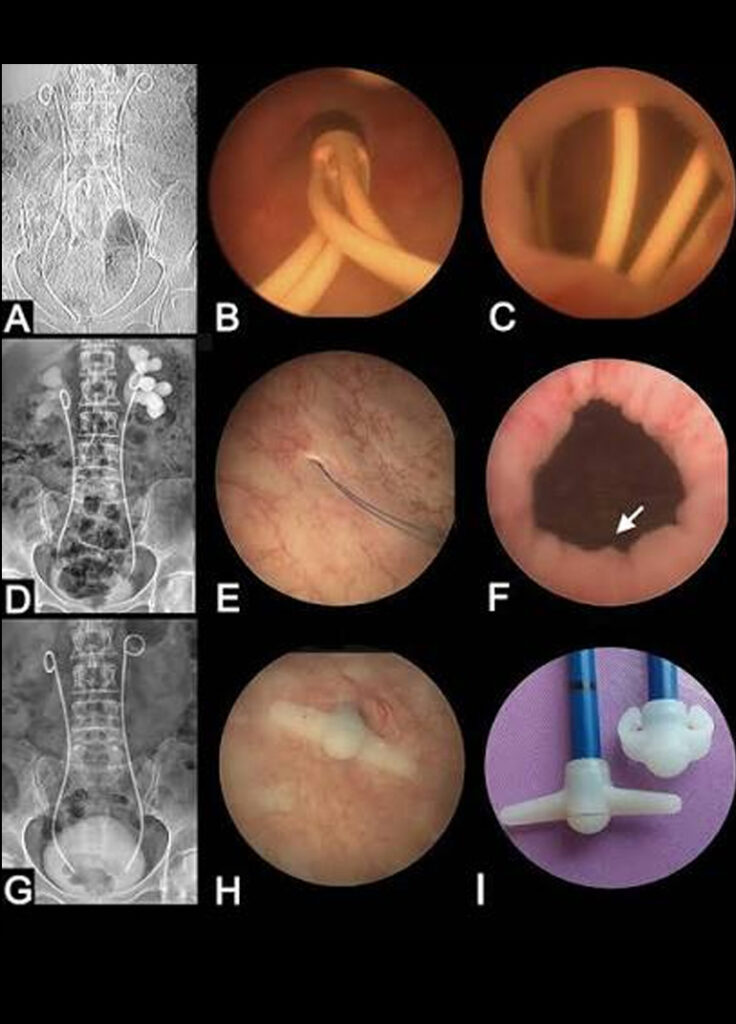
Methods: Clinical data from our institution, including outcomes for all ureteric stents inserted for long-term management of CUO from all causes from 2014 to 2017, were retrospectively reviewed and compared between the MS and PS episodes.
Results: A total of 247 stents were placed in 63 patients with CUO over the 4-year study period. Of these, 45 stents were MSs. There was no significant difference in all baseline characteristics between the MS and PS groups, except for the aetiology of obstructive cause. Mean indwelling stent duration was significantly greater for MS than for PS (228.6 ± 147.0 vs. 146.1 ± 66.0 days, P < 0.001), thereby leading to lower average number of stent changes per year in the MS group compared to the PS group (1.4 vs. 6.3 times, respectively). Despite the higher unit cost of MS compared to PS, there was no significant mean cost difference overall (cost per dwelling day SGD 7.82 ± SGD 10.44 vs. SGD 8.23 ± SGD 20.50, P = 0.888).
Robotic Guided Transperineal Prostate Biopsy: Our 10 Years’ Experience
Date: Sept 2018
Doctor Author: Du J, Lu YD, Law ZW, Ho HSS, Yuen JSP, Lee LS, Tay KJ, Chen K, Lau WKO BJU International, Sep 2018 (Supplement).
Presented at ERUS Marseilles 2018.
Research type- Conference abstract / 10-year single-centre clinical experience
Treatment area- Urology; robotic-guided transperineal prostate biopsy and prostate cancer diagnosis
Publication Summary
Methods: Clinical data including outcomes for all ureteric stents inserted for long-term management of CUO from all causes in our institution from 2014 to 2017 were retrospectively reviewed and compared between MS and PS episodes. Stent failure was defined as complication occurrence with obstruction, urosepsis or malposition with either type of stent in-situ. For cost analysis, we calculated the average cost of each inserted stent per indwelling day for both self-paying and co-paying government subsidised healthcare models. This took into account hospital and procedural charges, stent cost and indwelling duration of MS and PS stents with an arbitrary cut-off date of 1 Nov 2017 for stents that have yet to reach their due date for removal or change.
Results: A total of 247 stents were placed in 63 patients (mean age 61–13, Female n = 121 (49%)) over the 3 year study period. Of these, 18% (n = 45) were MS episodes and the remainder 82% (n = 202) were PS. 70% (n = 174) of stent insertion episodes were for malignant obstruction and 30% (n = 73) were for benign obstruction. For both malignant and benign CUO, there was no significant difference in age, race and obstructive cause between MS and PS stent groups but were different significantly in terms of gender. 66.7% (n = 30) of MS and 45.1% (n = 91) of PS were females, p = 0.009. In terms of outcomes for all causes of CUO, there was no significant difference in terms of operative time (29.0–21.1 vs. 28.7–30.1 minutes); creatinine change after stenting (3.88–23.68 vs. 0.43–58.74 μmol/L) and stent failure rates (n = 7 (15.6%) vs. n = 23 (11.4%)) between MS and PS groups respectively. Equivalent patency meant that the mean indwelling stent duration was significantly greater for MS than for PS (228.6–147.0 vs. 146.1–66.0 days, p < 0.0001) resulting in lower average stent change per patient of 1.4 and 6.3 respectively. Despite the higher cost of MS compared to PS (S$977.50 vs. S$195.50), there was no significant mean cost difference between MS and PS: mean cost respectively was S$14.55–13.16 and 14.02–11.60 (p = 0.9054) in self-paying patients and S$6.29–9.27 and 5.76–22.91 (p = 0.8939) for co-paying patients.

The role of subdermal suspension threads in elevation of the inframammary folds
Plastic and Reconstructive Surgery
Date: 2006
Doctor Author: Dr Shenthilkumar Naidu, Nanthini Kunaratnam, Cheong Ee Cherk, Jane Lim, T C Lim
Research type: Letter / clinical technique commentary
Treatment area; Plastic surgery, breast reconstruction, inframammary fold elevation using subdermal suspension threads
Long Head of the Triceps Transfer for Elbow Flexion
Plastic and Reconstructive Surgery
Date: 2007
Doctor Author: Dr Shenthilkumar Naidu, Aymeric Lim, Looi Kok Poh, V P Kumar
Research Type: Clinical technique article / reconstructive surgery case report
Treatment Area: Plastic and reconstructive surgery; upper limb reconstruction; elbow flexion restoration using long head of triceps transfer

Common benign and malignant neoplasms of the skin
Singapore Medical Journal
Date: 2008
Doctor Author: T W Shim, Dr Shenthilkumar Naidu, J Lim, T C Lim
Research Type: Review article
Treatment Area: Plastic and reconstructive surgery; skin cancer; diagnosis and clinical recognition of common benign and malignant skin neoplasms

The “hand-in-gloves” technique: vacuum-assisted closure dressing for multiple finger wounds
Journal of Plastic, Reconstructive & Aesthetic Surgery
Date: 2009
Doctor Author: Anthony Foo, Dr Shenthilkumar Naidu, Alphonsus Kin-Sze Chong
Research Type: Technical note / clinical technique article
Treatment Area: Plastic and reconstructive surgery; hand wounds; vacuum-assisted closure dressing for multiple finger wounds
Patent blue dye in lymphaticovenular anastomosis
Annals, Academy of Medicine, Singapore
Date: 2009
Doctor Author: Yan Lin Yap, Jane Lim, Timothy W H Shim, Dr Shenthilkumar Naidu, Wei Chen Ong, Thiam Chye Lim
Research Type: Case report / microsurgical technique article
Treatment Area: Plastic and reconstructive surgery; lymphoedema surgery; patent blue dye mapping for lymphaticovenular anastomosis
Publication Summary
Materials and methods: We describe a technique of performing lymphaticovenular anastomosis with patent blue dye enhancement. Our patient is a 50-year-old lady who suffers from chronic lymphoedema of the upper limb after mastectomy and axillary clearance for breast cancer 8 years ago.
Results: Patent blue dye is injected subdermally and is taken up readily by the draining lymphatic channels. This allows for easy identification of their course. The visualisation of the lumen of the lymphatic vessel facilitates microsurgical anastomosis. The patency of the anastomosis is also demonstrated by the dynamic pumping action of the lymphatic within the vessels.
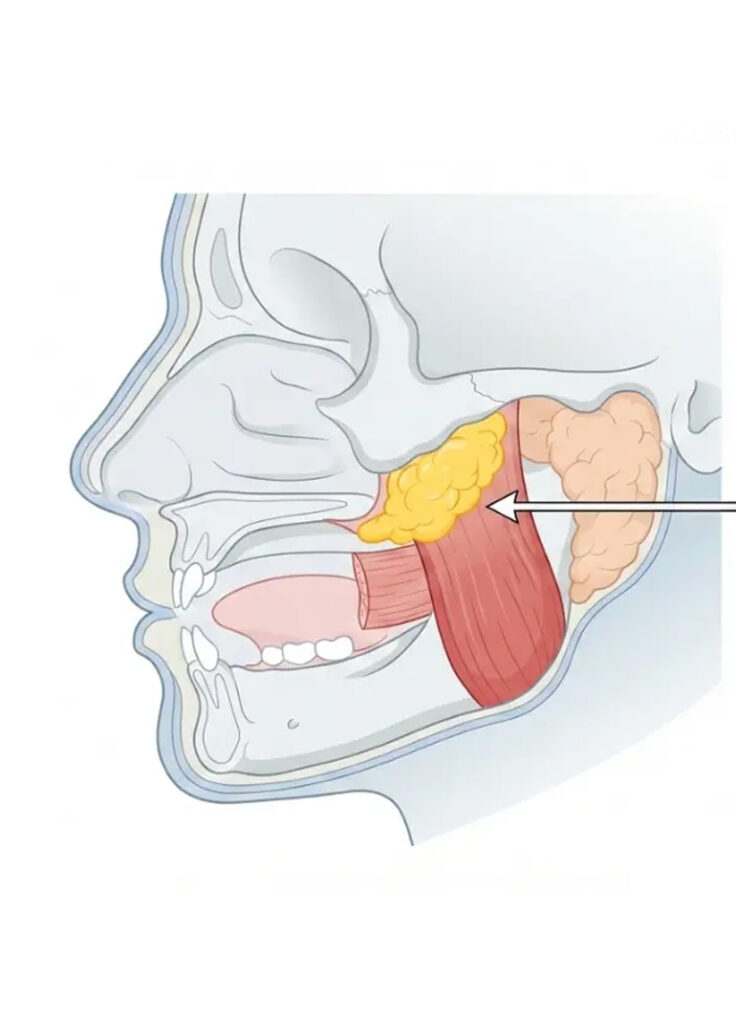
Plastic and Reconstructive Surgery
Date: 2010
Doctor Author: Jeong Tae Kim, Dr Shenthilkumar Naidu, Youn Hwan Kim
Research Type: Case report / reconstructive surgery technique article
Treatment Area: Plastic and reconstructive surgery; parotidectomy reconstruction; buccal fat flap for Frey syndrome prevention and facial contouring
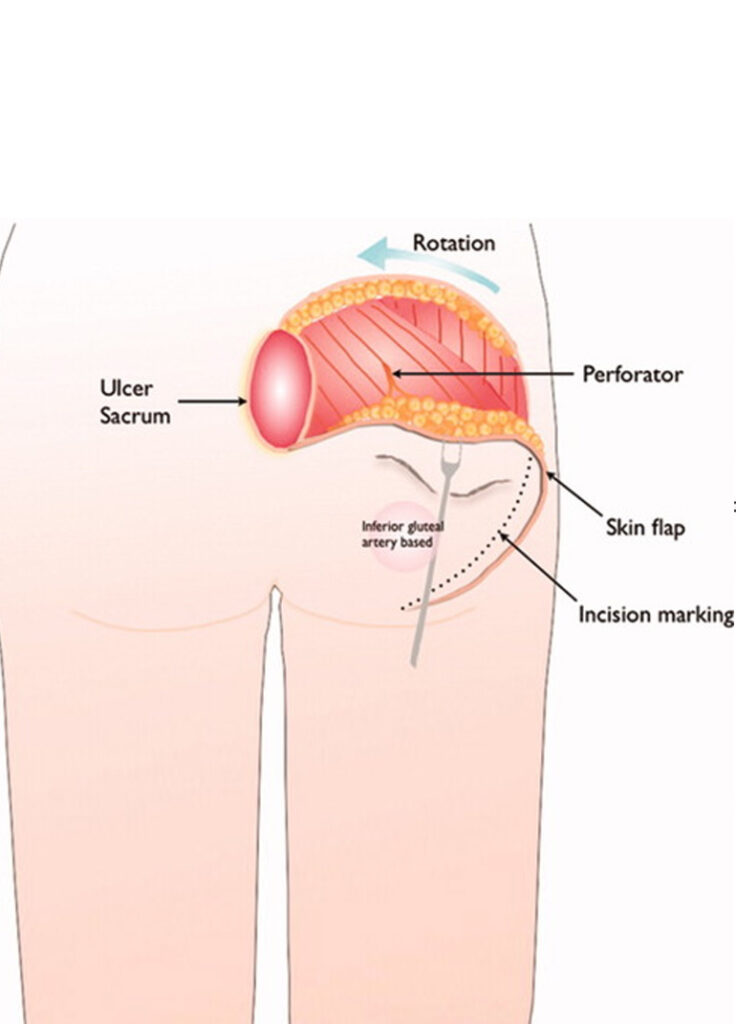
Plastic and Reconstructive Surgery
Date: 2010
Doctor Author: Jeong Tae Kim, Dr Shenthilkumar Naidu, Youn Hwan Kim
Research Type: Clinical technique article / reconstructive flap design study
Treatment Area: Plastic and reconstructive surgery; buttock defect reconstruction; gluteus maximus perforator-based island flap design
Publication Summary
Methods: After excisional débridement of the lesion, a perforator adjacent to the defect is selected. The tissue of the donor region is pinched to simulate closure. The change in shape of the recipient defect is noted and the dimensions of this new shape are measured. This will serve as the new dimensions of the donor tissue. The tissue components required to fill the defect are then analyzed and the flap is raised. It can be either muscle-sparing, muscle-splitting, or muscle-inclusive. A 1- to 2-cm diameter of soft tissue around the perforator is preserved. The flap is islanded and transposed, and the donor site is closed primarily, acting as a “locking barrier” to the flap. Tension-free closure of the recipient flap is then carried out. Seventy-five patients underwent closure of varying defects of the gluteal region using this technique.
Results: The authors had a total of three minor complications. The rest of the patients healed well, with no recurrence at a mean follow-up of 15 months.
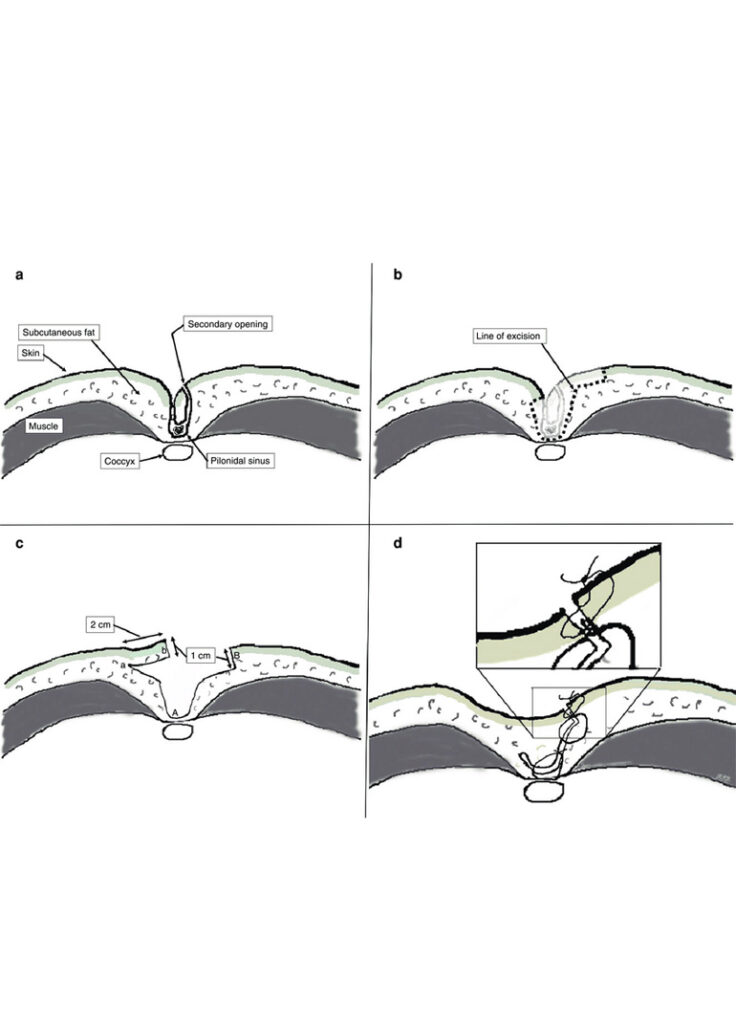
A perforator solution for excisional defects of pilonidal sinus
Journal of Plastic, Reconstructive & Aesthetic Surgery
Date: 2010
Doctor Author: Youn Hwan Kim, Dr Shenthilkumar Naidu, Chang Yeon Kim, Kang Hong Lee, Jeong Tae Kim
Research Type: Case report / reconstructive flap technique article
Treatment Area: Plastic and reconstructive surgery; pilonidal sinus reconstruction; perforator flap coverage for excisional defects
Plastic and Reconstructive Surgery
Date: 2010
Doctor Author: Chang Yeon Kim, Dr Shenthilkumar Naidu, Youn Hwan Kim
Research Type: Clinical study / reconstructive microsurgery case series
Treatment Area: Plastic and reconstructive surgery; lower limb reconstruction; supermicrosurgical free flap coverage for foot defects caused by occlusive vascular disease
Publication Summary
Methods: After excisional débridement of the wound, under loupe magnification, branches of the terminal foot vessels were sought. Once identified and deemed suitable, the thin peroneal flaps were isolated based on perforator vessels. The flaps raised were either peroneal perforator-based or soleus perforator-based flaps. Microanastomosis was performed at the perforator level with 10-0 or 11-0 Ethilon sutures, and the flap was inset. The donor site was closed primarily.
Results: A total of 18 such flaps were raised in 17 patients with 15 septocutaneous and three musculocutaneous perforators. Sixteen peroneal perforator-based flaps and two soleus perforator-based flaps were used. There was one major (flap loss) and two minor (wound dehiscence) complications. The rest of the patients healed well, with no recurrence at a mean follow-up of 8.3 months.

The “Taiwanese giant”: hormonal and genetic influences in fibrous dysplasia
Annals of Plastic Surgery
Date: 1998
Doctor Author: P Szwajkun, Dr Vincent Yeow, A F Breidahl
Research Type: Case report / clinical genetics commentary
Treatment Area: Plastic and reconstructive surgery; craniofacial and skeletal deformity; fibrous dysplasia with hormonal and genetic influences
Publication Summary
Abstract: A 14-year-old boy has been followed for 4 years with a rapidly growing, recurrent area of fibrous dysplasia of the left maxilla and zygoma following resection and bone grafting. Standing 190 cm tall, he was found to have elevated serum growth hormone levels and a pituitary adenoma. His case appears to represent a postzygotic gene mutation of McCune-Albright syndrome. It is possible that the elevated growth hormone levels are in part responsible for the rapid progression of the tumor.
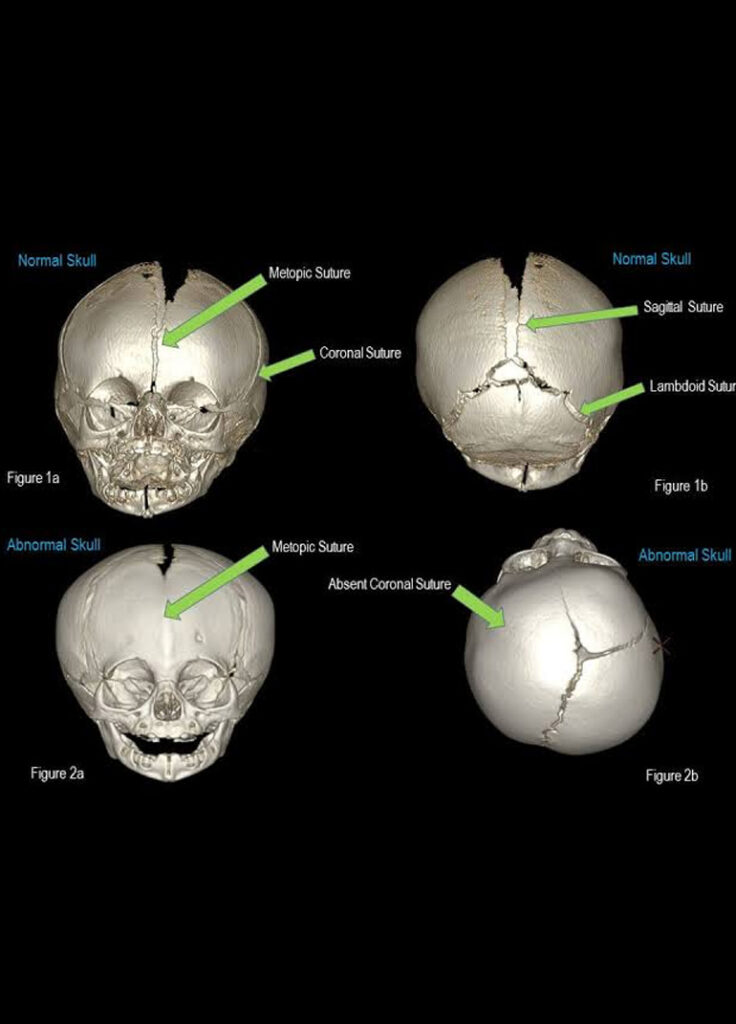
Effect of cranial suture autotransplantation from metopic to coronal suture
Journal of Craniofacial Surgery
Date: 1998
Doctor Author: Dr Vincent Yeow, W T Wu
Research Type: Animal study / craniofacial surgical research
Treatment Area: Plastic and reconstructive surgery; craniofacial surgery; cranial suture transplantation and craniosynostosis research
Publication Summary
Abstract: The aim of this study was to determine the outcome of autotransplanting part of the metopic suture to a defect in the coronal suture in a pig model and to explore further the concept of functioning and nonfunctioning recipient sites. The authors harvested 15-mm x 10-mm bone grafts, incorporating a part of the metopic suture, in 10 Yorkshire pigs under general anesthesia. The authors immediately autotransplanted the grafts to a surgically created defect along the line of the coronal suture. Both donor and graft were either covered with pericranium or left bare. Radiopaque titanium markers were inserted to assess growth 1) of the transplanted suture; 2) across both coronal sutures; and 3) across the metopic suture. Serial radiographs were taken immediately after surgery and at 3-week intervals. The pigs were then killed at 21 weeks. The cranium was harvested, and blocks of donor site and graft were taken, incorporating the embedded titanium markers. Histologic analysis confirmed graft take in all pigs. All grafts continued to function as active cranial sutures with no growth disturbance compared with the contralateral coronal suture (P = 0.953). There was also regeneration of the donor defect, as confirmed by histologic analysis, with no growth disturbance across the metopic suture (P = 0.972). Pericranium did not alter graft take or subsequent growth (P = 0.964). However, pericranium resulted in a much smaller defect (P = 0.045). These results show that after autotransplanting a cranial suture to replace another cranial suture, the graft continues to grow and function as a cranial suture to meet the functional demands of the new recipient site. Pericranium has a significant effect on calvarial regeneration but does not affect cranial suture autotransplantation.
Annals of Plastic Surgery
Date: 1998
Doctor Author: P K Chen, S C Chang, F Huang, Y R Chen, Dr Vincent Yeow, W G Williams
Research Type: Case report / craniofacial surgical technique article
Treatment Area: Plastic and reconstructive surgery; craniofacial surgery; transzygomatic coronoidectomy for trismus caused by mandibular coronoid process osteochondroma
Publication Summary
Abstract: Osteochondroma is the most common benign tumor of the skeletal system. In the craniofacial skeleton, however, osteochondroma is uncommon. Even more rare is osteochondroma of the coronoid process. A review of the literature reveals only 31 reported cases of osteochondroma of the coronoid process of the mandible. The preponderance of patients were young men (67.7%) and most presented with a facial deformity. As a benign tumor, the problems with surgical treatment have dealt with the inaccessibility of the lesion and hence the surgical approach of choice. The previous surgical approaches have either been intraoral, external, or a combination of both. We present a transzygomatic approach via a coronal incision that gives excellent access and a good cosmetic result, and protects the facial nerve from damage.
Annals of Plastic Surgery
Date: 1999
Doctor Author: Philip K. T. Chen, Dr Vincent Yeow, M. Samuel Noordhoff, Yu-Ray Chen
Research Type: Prospective clinical study
Treatment Area: Plastic and reconstructive surgery; cleft lip and nasal reconstruction; nasal floor augmentation using Surgicel during primary lip repair
Publication Summary
Abstract:
The symmetry of the alar base and the nasal floor is very important in achieving a satisfactory result in primary lip and nasal reconstruction during cleft lip repair. The skeletal base of the nasal pyramid is usually hypoplastic even in incomplete clefts. A periosteal pocket filled with Surgicel can facilitate blood clot formation and can theoretically stimulate bone formation, thereby improving the asymmetry of the bone base. To test this hypothesis, a prospective study was performed in 64 primary lip repairs by comparing the effect of subperiosteal nasal floor augmentation with Surgicel. From February 1989 to June 1993, 64 patients with incomplete cleft lips (excluding occult cleft lip and complete clefts with Simonart’s band) were operated by the same surgeon. The patients were divided randomly into two groups. One group had subperiosteal nasal floor augmentation with Surgicel and the other group did not. The lip repair was a rotation-advancement cheiloplasty with primary closed rhinoplasty of the tip and ala. In the first group, a subperiosteal pocket was created under the cleft alar base and the nasal floor. The pocket was filled with Surgicel up the point where the level of the alar base and the nasal floor was symmetrical with the noncleft side. The control group underwent a similar procedure, less the creation of the subperiosteal pocket and the use of Surgicel. All patients were followed for at least 3 years and their photographs were used to compare and analyze the results of their nasal correction. Critical attention was paid to the symmetry of their nasal floor and alar base. The results were evaluated by at least two plastic surgeons for consistency. The data indicate that the control group showed a higher number of subjects with asymmetry (10 of 32) compared with the study group (8 of 32). However, there was no statistical significance to the findings. Two patients in the study group who received Surgicel developed hypertrophic lip scars. This study, although unable to determine statistically the contributory affect of Surgicel in primary nasal reconstruction, does show a possible benefit from the use of osteogenic materials in the primary management of the deficient nasal floor. Hypertrophic scars developed by 2 patients in the study group may point to a possible soft-tissue reaction to the use of Surgicel in primary lip and nasal repair.

Cleft lip scar camouflage using dermal micrografts
Plastic and Reconstructive Surgery
Date: 1999
Doctor Author: Yu-Ray Chen, Dr Vincent Yeow
Research Type: Clinical technique article / case series
Treatment Area: Plastic and reconstructive surgery; cleft lip scar revision; dermal micrografts for scar camouflage
Publication Summary
Abstract: The use of dermal micrografts to camouflage cleft lip scars is a simple and effective method. We have used dermal micrografts, some hair-bearing, to camouflage hypopigmented scars in 10 patients. This method improves the colour of the scar, corrects wound distortion and direction to a certain degree, and enables the resultant scar to blend into the adjacent tissue more naturally. Unlike with other methods of scar revision, additional tissue is not sacrificed and new incision lines are not created.
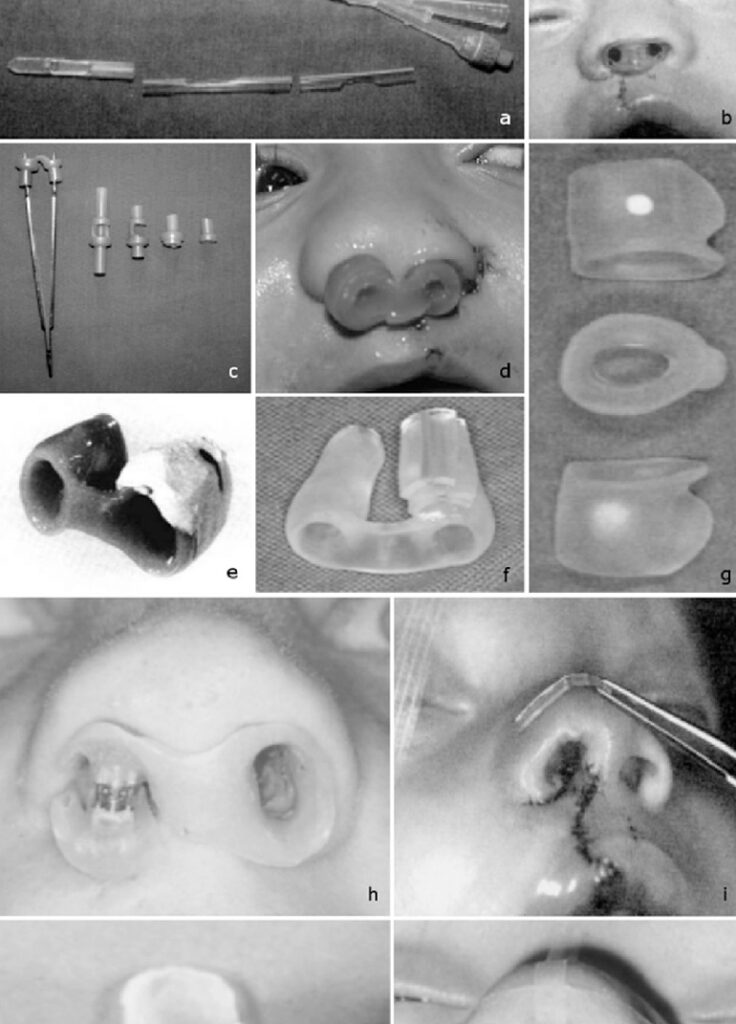
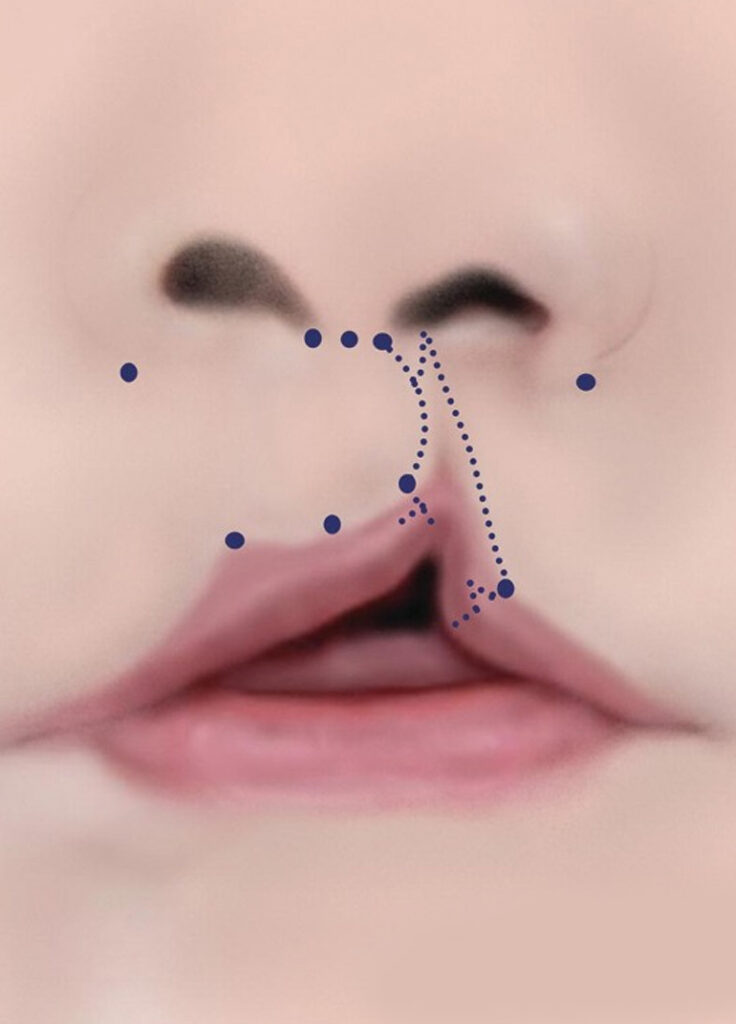
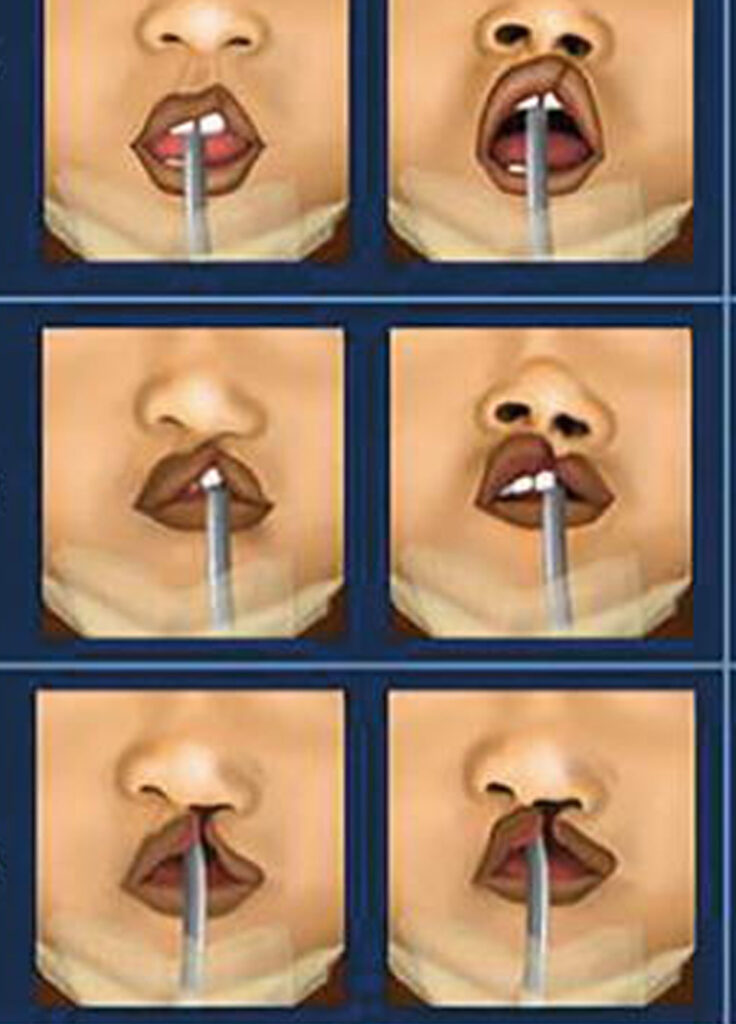
The use of nasal splints in the primary management of unilateral cleft nasal deformity
Plastic and Reconstructive Surgery
Date: 1999
Doctor Author: Dr Vincent Yeow, Philip K. T. Chen, Yu-Ray Chen, Samuel M. Noordhoff
Research Type: Prospective clinical study
Treatment Area: Plastic and reconstructive surgery; cleft lip and nasal reconstruction; postoperative nasal splinting for unilateral cleft nasal deformity
Publication Summary
Abstract: Primary surgical correction of the cleft lip nasal deformity is routinely performed at the Craniofacial Center at Chang Gung Memorial Hospital. Over time, however, there is a tendency for the lower lateral cartilage to retain its memory and, subsequently, recreate the preoperative nasal deformity. Therefore, it is current practice to use a nostril retainer for a period of at least 6 months to maintain the corrected position of the nose. The aim of this study was to qualitatively assess the benefit of postoperative nasal splinting in the primary management of unilateral cleft nasal deformity. Data from two groups of 30 patients with complete unilateral cleft lips each were retrospectively collected and analyzed. The first group served as a control (no nasal splints), and the second group used the nasal retainer compliantly for at least 6 months postoperatively. All patients had their primary lip repair at 3 months of age. A photographic evaluation of the results when the patients were between 5 and 8 years of age was conducted. The parameters used to assess the nasal outcome were nostril symmetry, alar cartilage slump, alar base level, and columella tilt. The first scores were based on residual nasal deformity, and the second set were based on overall appearance. It was found that the mean scores of residual nasal deformity for all four parameters in patients who used the nasal stent were statistically better than the scores of patients who did not (p values ranged from 0.0001 to 0.005). The overall appearance scores for the four parameters in the patients who used the nasal stent after surgery were also statistically better than the scores for those who did not (p values ranged from 0.0001 to 0.01). The results show that postoperative nasal splinting in the primary management of the unilateral cleft nasal deformity serves to preserve and maintain the corrected position of the nose after primary lip and nasal correction, resulting in a significantly improved aesthetic result. Therefore, it is recommended that all patients undergoing primary correction of complete unilateral cleft deformity use the nasal retainer postoperatively for a period of at least 6 months.
Orthognathic surgery in craniomaxillofacial fibrous dysplasia
Journal of Craniofacial Surgery
Date: 1999
Doctor Author: Dr Vincent Yeow, Y R Chen
Research Type: Case report / craniofacial surgical technique article
Treatment Area: Plastic and reconstructive surgery; craniofacial surgery; orthognathic surgery for craniomaxillofacial fibrous dysplasia
Publication Summary
Abstract: In craniomaxillofacial fibrous dysplasia, jaw involvement often causes facial asymmetry, an occlusal cant, and loss of teeth. Although conservative management of fibrous dysplasia affecting the jaws is widely practiced, orthognathic surgery is indicated in such cases to restore occlusion and correct dentofacial deformity brought on by the disease process. Since 1981, the Craniofacial Center at Chang Gung Memorial Hospital in Taiwan has treated a total of 84 patients with craniomaxillofacial fibrous dysplasia. Of these, 55 (65%) had fibrous dysplasia affecting the jaws (Zone 4). Between 1988 and 1997, orthognathic surgery was performed on 1 male and 4 female patients with fibrous dysplasia involving the teeth-bearing jaws. One patient had localized fibrous dysplasia that involved the mandible. The other 4 patients had polyostotic craniofacial involvement of Zones 1, 2, or 3 and 4A. The patient with isolated mandibular involvement and 2 patients with maxillary fibrous dysplasia had single-jaw surgery. The other 2 patients with maxillary involvement required simultaneous two-jaw surgery to correct the dentofacial deformities resulting from the disease process. Follow-up ranged from 12 months to 9 years. All the patients had stable occlusion, good facial aesthetics, and no further recurrence after surgery. The long-term stability of the achieved occlusion and facial appearance confirms that adequate healing in fibrodysplastic bone is to be expected using the standard fixation.
A Review of Mandibular Fractures in a Craniomaxillofacial Trauma Centre
Annals, Academy of Medicine, Singapore
Date: 1999
Doctor Author: A G Tay, Dr Vincent Yeow, B K Tan, K Sng, M H S Huang, C L Foo
Research Type: Original article / retrospective clinical review
Treatment Area: Plastic and reconstructive surgery; craniomaxillofacial trauma; mandibular fracture patterns, management and outcomes
Publication Summary
Abstract: This report is a retrospective review of 74 cases of mandibular fractures managed in a craniomaxillofacial trauma centre between January 1994 and May 1998. Demographic data revealed that 85% of the patient population were male, with a mean age of 27.5 years. The commonest causes of injury were motor vehicle accidents (48.6%), followed by assault (16.2%) and accidental falls (17.6%). In 25 patients (33.8%) the fractures were single. Of these, fractures of the condylar region were the most common (8 patients). The remaining patients sustained fractures in two or more anatomic sites. There were other associated facial fractures in 45.9% of patients. Trauma to other systems was present in 37.8%, with orthopaedic and neurosurgical injuries being the most common. Surgical management in the form of open reduction and internal fixation was carried out in 61 patients (82.4%). Maxillo-mandibular fixation was used as an adjunct to maintain occlusion and bony reduction in unstable and comminuted fractures (15 patients, 20.3%), and as the primary mode of treatment in patients with stable, undisplaced fractures, particularly condylar fractures, in which the pretraumatic occlusal relationship was not disrupted (9 patients, 12.2%). A successful outcome was defined as a stable and healed fracture, with restoration of functional occlusion, facial symmetry and facial aesthetics. Complications observed included temporomandibular joint dysfunction (10.8%), malocclusion (9.5%), infection (8.1%), implant exposure (5.4%), and non-union or delayed union (4.1%).
Epidemiology of cleft lip and palate in Singapore
Annals, Academy of Medicine, Singapore
Date: 1999
Doctor Author: N N Yi, Dr Vincent Yeow, S T Lee
Research Type: Hospital-based epidemiological study
Treatment Area: Plastic and reconstructive surgery; cleft lip and palate; epidemiology and clinical patterns of cleft deformities in Singapore
Publication Summary
Abstract: During the study period from January 1985 to December 1994, there were 1105 new cleft cases seen in the Department of Plastic Surgery, Singapore General Hospital. These included newborn as well as unoperated children and adult cases. During the same period, the total number of recorded births in Singapore was 474,542. Out of the 1105 new cleft cases seen, 984 were Singaporeans. The incidence of this hospital-based study of cleft population in Singapore was 2.07 per 1000 livebirths. Chinese had the highest incidence of 1.64 per 1000 as compared to Malay, Indian and other races. The most common type of cleft deformity was complete cleft lip and palate. The left side was found to be more affected than the right side in all types of cleft deformity. There was no significant difference in sex distribution; the male to female ratio was 1.1:1. However, females had a higher incidence of cleft palate than males. Associated congenital deformities occurred in 1.5% of the total cleft population.
The role of multiple-segment osteotomies in orthognathic surgery
Annals, Academy of Medicine, Singapore
Date: 1999
Doctor Author: Dr Vincent Yeow, Y R Chen, C P Su
Research Type: Clinical study / retrospective case series
Treatment Area: Plastic and reconstructive surgery; craniofacial surgery; multiple-segment osteotomies for dentofacial deformities and malocclusion
Publication Summary
Abstract:Multiple segment orthognathic (MSO) surgery is an effective approach to deal with a wide range of dento-facial deformities that have occlusal problems. The indications for MSO surgery were patients with dentofacial deformities and malocclusion requiring stable correction within a short overall treatment period. From 1991 to 1998, 107 patients had MSO orthognathic procedures done at Chang Gung Memorial Hospital for maxillary protrusion/deformity (34 cases), maxillary protrusion and mandibular prognathism (69 cases), and non-cleft maxillary retrusion (4 cases). Follow up period ranged from 6 months to 7 years and results showed stability in movements with only 3 complications. The average overall treatment time was approximately 15 months. Our experience with 107 consecutive patients have shown the results of MSO surgery to be good and the procedure safe with no tooth or segment loss.
Midface distraction osteogenesis in cleft patients: a case report
Annals, Academy of Medicine, Singapore
Date: 1999
Doctor Author: Dr Vincent Yeow, P K Chen, W Y Lin, C Yun
Research Type: Case report / craniofacial surgical technique article
Treatment Area: Plastic and reconstructive surgery; craniofacial surgery; midface distraction osteogenesis for cleft-related maxillary hypoplasia
Publication Summary
Abstract: We present a case of midface distraction in a bilateral cleft lip and palate patient. The patient was a 10-year-old who underwent a high LeFort I osteotomy followed by placement of the Rigid External Distraction halo. Distraction was commenced on the fifth postoperative day at a rate of 1 to 1.5 mm per day until a total of 17 mm of maxillary advancement had been achieved. There were no complications and follow up was at 9 months post distraction. Results show that the patient had improved facial aesthetics and dental occlusion which was overcorrected to a Class III relationship. Velopharyngeal function was unaffected. Distraction osteogenesis of the midfacial skeleton in cleft patients offers the possibility to remodel not only the underlying bony skeleton but also all the soft tissues of the face and palate.
Multiple-segment osteotomy in maxillofacial surgery
Plastic and Reconstructive Surgery
Date: 1999
Doctor Author: Y R Chen, Dr Vincent Yeow
Research Type: Clinical study / maxillofacial surgical technique article
Treatment Area: Plastic and reconstructive surgery; maxillofacial surgery; multiple-segment osteotomy for correction of dentofacial deformities
Publication Summary
Abstract: We present a case of midface distraction in a bilateral cleft lip and palate patient. The patient was a 10-year-old who underwent a high LeFort I osteotomy followed by placement of the Rigid External Distraction halo. Distraction was commenced on the fifth postoperative day at a rate of 1 to 1.5 mm per day until a total of 17 mm of maxillary advancement had been achieved. There were no complications and follow up was at 9 months post distraction. Results show that the patient had improved facial aesthetics and dental occlusion which was overcorrected to a Class III relationship. Velopharyngeal function was unaffected. Distraction osteogenesis of the midfacial skeleton in cleft patients offers the possibility to remodel not only the underlying bony skeleton but also all the soft tissues of the face and palate.
Combining single- and double-tooth osteotomies with traditional orthognathic surgery
Journal of Craniofacial Surgery
Date: 1999
Doctor Author: Dr Vincent Yeow, Yu-Ray Chen, Chih-Peng Su
Research Type: Clinical technique article / maxillofacial surgical commentary
Treatment Area: Plastic and reconstructive surgery; maxillofacial surgery; single-tooth and double-tooth osteotomies combined with traditional orthognathic surgery
Publication Summary
Abstract: Combining large-segment orthognathic surgery and unitooth or small-segment surgery is an effective approach to deal with a wide range of dentofacial deformities that have minor to severe occlusal problems. The indications for combining single- or double-tooth osteotomies with traditional orthognathic surgery were patients with dentofacial deformities and malocclusion requiring stable correction within a short overall treatment period. From 1991 to 1998, a total of 36 patients underwent combination single- or double-tooth-segment osteotomy with traditional orthognathic procedures performed at Chang Gung Memorial Hospital. The indications for surgery were maxillary protrusion (N = 5), bimaxillary protrusion (N = 19), mandibular prognathism with maxillary protrusion (N = 11), and noncleft maxillary retrusion (N = 1). The types of osteotomies performed were the Le Fort I, the anterior segmental osteotomies of the maxilla or the mandible, the palatal split, and the posterior segment in combination with single-tooth or double-tooth segments. Follow-up ranged from 12 months to 6 years and showed stability in the movements with no complications. There was no loss of any “osteotomized” segment. The average overall treatment time was approximately 18 months–5 months preoperative and 13 months postoperative orthodontic treatment. This was at least 6 months shorter in duration compared with traditional orthognathic surgery. Combining traditional orthognathic surgery with single- or double-tooth segments allows us to treat complex dentofacial deformities in the vertical, transverse, and sagittal dimensions with differential repositioning of all segments, either major or minor, simultaneously. The authors’ experience with 36 consecutive patients evidence good results and demonstrate the procedure to be safe with minimal complications.
Journal of Cranio-Maxillofacial Surgery
Date: 2001
Doctor Author: D Rohner, B K Tan, C Song, Dr Vincent Yeow, B Hammer
Research Type: Clinical case series / reconstructive surgical technique article
Treatment Area: Plastic and reconstructive surgery; craniofacial reconstruction; repair of composite zygomatico-maxillary defects using free bone grafts and free vascularized tissue transfer
Publication Summary
Methods: The key points of this technique are: (1) precise reconstruction of the zygomatico-maxillary complex including the orbit; (2) creation of a skeletal framework for canthopexy and suspension of the free flap; (3) repair of through-and-through soft tissue defects with a folded musculocutaneous free flap; and (4) simultaneous harvesting and reconstruction using two surgical teams to reduce the duration of surgery.
Results: Reconstruction of the zygomatico-maxillary complex could be successfully accomplished in a single surgical procedure.
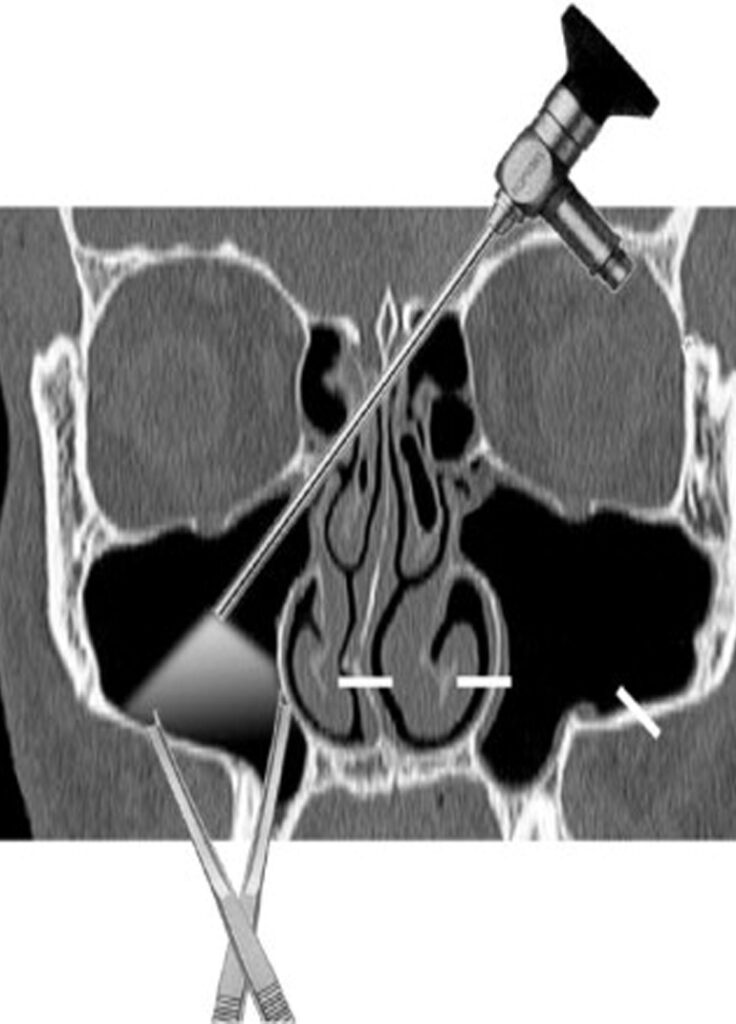
Endoscopically assisted Le Fort I osteotomy
Journal of Cranio-Maxillofacial Surgery
Date: 2001
Doctor Author: Dennis Rohner, Dr Vincent Yeow, Beat Hammer
Research Type: Cadaveric surgical study / minimally invasive craniofacial surgical technique article
Treatment Area: Plastic and reconstructive surgery; craniofacial and orthognathic surgery; endoscopically assisted Le Fort I osteotomy
Publication Summary
Methods: Four vertical incisions were used in the vestibule (paranasally and posteriorly) as approaches. The endoscope allowed direct visualization of the osteotomy of the maxilla including the pterygomaxillary junction. The osteotomies could be accomplished with a straight 4 mm osteotome for medial and lateral antral walls and nasal septum and a curved osteotome for the pterygomaxillary junction.
Results: The procedures were successful. The descending palatal arteries could be preserved in all cases as a result of endoscopic control. Rigid fixation of the downfractured maxillae was carried out using self-drilling titanium screws and plates.
International Task Force on Volunteer Cleft Missions
Journal of Craniofacial Surgery
Date: 2002
Doctor Author: Dr Vincent Yeow, S T Lee, T J Lambrecht, J Barnett, M Gorney, W Hardjowasito, G Lemperle
Research Type: Task force report / international consensus guidance
Treatment Area: Plastic and reconstructive surgery; cleft lip and palate surgery; standards and recommendations for international volunteer cleft missions
Publication Summary
Abstract: The International Task Force on Volunteer Cleft Missions was set up to provide a report to be presented at the Eighth International Congress of Cleft Palate and Associated Craniofacial Anomalies on September 12, 1997, in Singapore. The aim of the report was to provide data from a wide range of different international teams performing volunteer cleft missions and, thereafter, based on the collected data, to identify common goals and aims of such missions. Thirteen different groups actively participating in volunteer cleft missions worldwide were selected from the International Confederation of Plastic and Reconstructive Surgery’s list of teams actively participating in volunteer cleft missions. Because of the time frame within which the committee had to work, three groups that did not respond by the stipulated deadline were omitted from the committee. The represented members and their respective institutions have undertaken more than 50 volunteer cleft missions to underdeveloped nations worldwide within the last 3 years. They have visited over 20 different countries, treating more than 3,500 patients worldwide. Based on the data collected and by consensus, the committee outlined recommendations for future volunteer cleft missions based on 1) mission objectives, 2) organization, 3) personal health and liability, 4) funding, 5) trainees in volunteer cleft missions, and 6) public relations. The task force believed that all volunteer cleft missions should have well-defined objectives, preferably with long-term plans. The task force also decided that it was impossible to achieve a successful mission without good organization and close coordination. All efforts should be made, and care taken, to ensure that there is minimal morbidity and no mortality. Finally, as ambassadors of goodwill and humanitarian aid, the participants must make every effort to understand and respect local customs and protocol. The main aims are to provide top-quality surgical service, train local doctors and staff, develop and nurture fledgling cleft programs, and, finally, make new friends.
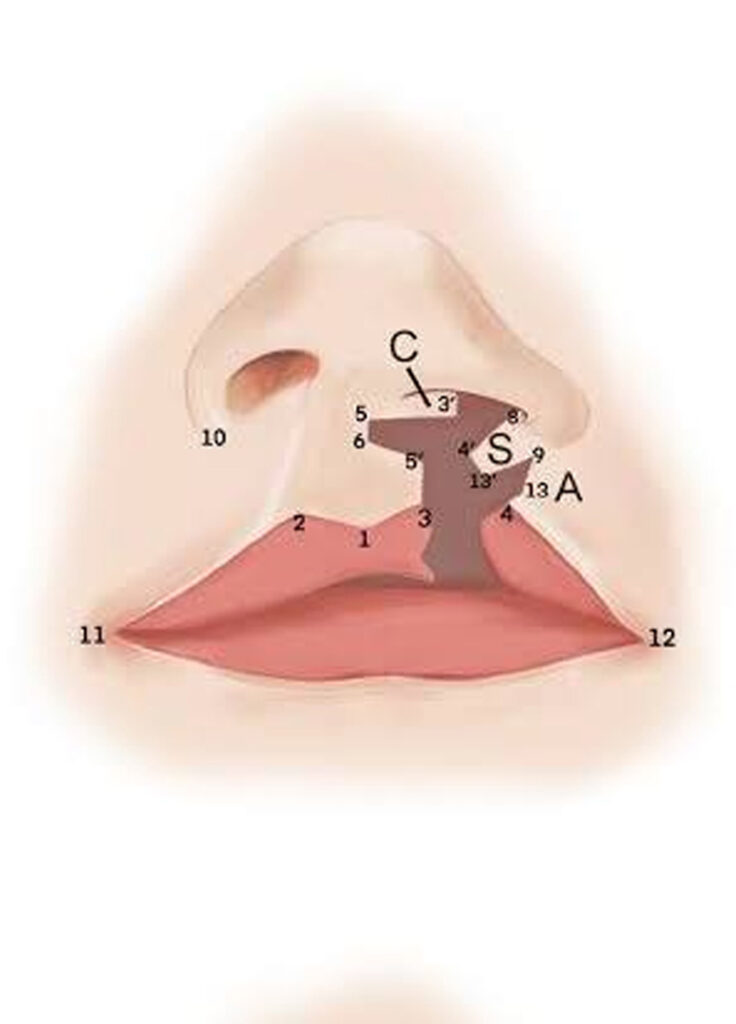
An anthropometric analysis of indices of severity in the unilateral cleft lip
Journal of Craniofacial Surgery
Date: 2002
Doctor Author: Dr Vincent Yeow, M H S Huang, S T Lee, S M C Fook Chong
Research Type: Prospective anthropometric clinical study
Treatment Area: Plastic and reconstructive surgery; cleft lip and palate surgery; anthropometric assessment of unilateral cleft lip severity
Publication Summary
Abstract: The aim of this study was to analyze the relationships among three key anthropometric parameters in the unilateral cleft lip to determine the correlations, if any, among these indices of severity. Using a standardized anthropometric documentation protocol, preoperative measurements of 125 unilateral cleft lips (103 complete and 22 incomplete) were performed under general anesthesia by a single surgeon at the time of primary lip repair at the age of 3 months. The following key measurements were analyzed statistically: (1) the philtral height difference (PHD) between the cleft and noncleft sides, (2) the nasal floor width difference (NFWD) between the cleft and noncleft sides, and (3) the cleft width (CW). The mean values of all three indices were greater in the complete group versus the incomplete group. These differences were statistically significant. Linear relationships were obtained between NFWD and GAP, between PHD and GAP, and between PHD and NFWD in the complete group. In contrast, the relationships between PHD and GAP, and between PHD and NFWD were nonlinear in the incomplete group. These findings suggest that there was a strong correlation between the transverse and vertical tissue deficiencies in the complete cleft lip. In incomplete clefts, however, this correlation did not exist. In other words, the incomplete cleft lip can be associated with a severely short philtrum even in the presence of a relatively mild transverse tissue deficit. Therefore, it is not necessarily easier to repair an incomplete cleft lip in terms of the correction of the vertical tissue deficiency
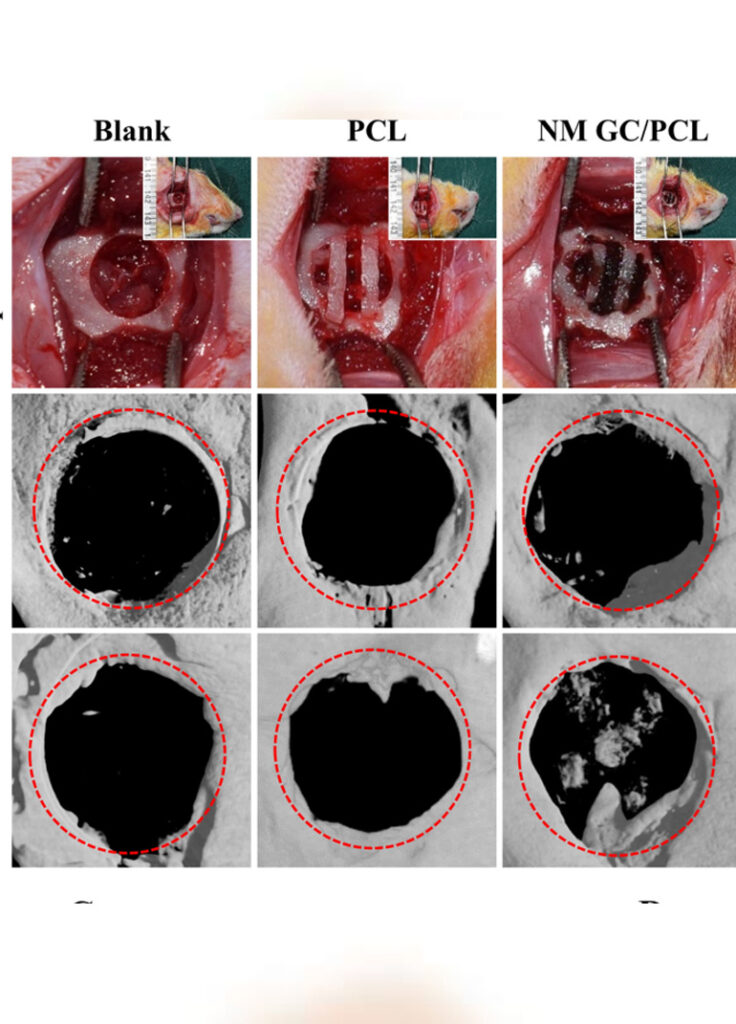
Cranio-Maxillofacial Surgery
Date: 2002
Doctor Author: D Rohner, D W Hutmacher, P See, K C Tan, Dr Vincent Yeow, S Y Tan, S T Lee, B Hammer
Research Type: Experimental animal study / biomaterials reconstruction study
Treatment Area: Plastic and reconstructive surgery; craniofacial reconstruction; CAD-CAM designed bioresorbable polycaprolactone framework for craniofacial defect repair
Publication Summary
Methods: Twenty orbital defects (2 x 2 cm) were created in ten adult Yorkshire pigs. Two software products (Velocity and Mimix) were evaluated with regard to image processing, three-dimensional reconstruction, and fabrication of individually shaped polycaprolactone (PCL) scaffolds to reconstruct these defects. Four different techniques were tested for the reconstruction: group 1 = no reconstruction, group 2 = polylactide sheet, group 3 = PCL scaffold, group 4 = bone marrow-coated PCL scaffold. The pigs were sacrificed at 3 months.
Results: In group 1 soft tissue scar formation could be found, but without any new bone. Group 2 showed a thick fibrous capsule around the PLLA sheet, whereas at the border zone of the defect signs of new bone formation could be detected. In group 3 the PCL scaffolds were filled with fibrous tissue and some areas that showed new bone formation (6.4% of the area of the defect). In group 4 the new bone formation (17.8% of the area of the defect) was significantly higher in quantity than in group 3.
Endoscopically assisted Le Fort 1 osteotomy: a study in human cadaver heads
Mund-, Kiefer- und Gesichtschirurgie
Date: 2003
Doctor Author: D Rohner, Dr Vincent Yeow, B Hammer
Research Type: Cadaveric surgical study / minimally invasive craniofacial surgical technique article
Treatment Area: Plastic and reconstructive surgery; craniofacial and orthognathic surgery; endoscopically assisted Le Fort I osteotomy in human cadaver heads
Publication Summary
Methods and results: Endoscopically assisted Le Fort 1-osteotomy was performed in a cadaver study with six human skulls. Vertical incisions were used to approach the maxilla using the endoscope. The bone cuts could be carried out with a 4-mm osteotome preserving the buccal mucosa. The downfracture of the maxilla was accomplished without damaging the descending palatal arteries, which could be verified endoscopically. Rigid fixation was performed using 1.5-mm titanium plates (Synthes, Mathys AG, Bettlach, Switzerland) and self-drilling screws.
Discussion: This cadaver study showed that the Le Fort 1 osteotomy could be carried out through limited approaches using endoscopic techniques and self-drilling fixation tools. Further experimental work and improvements will help to introduce this technique into clinical application.
Endoscopic approaches to maxillary orthognathic surgery
Facial Plastic Surgery Clinics of North America
Date: 2006
Doctor Author: D Rohner, Dr Vincent Yeow
Research Type: Review article / minimally invasive craniofacial surgical technique review
Treatment Area: Plastic and reconstructive surgery; craniofacial and orthognathic surgery; endoscopic approaches to maxillary orthognathic surgery
Publication Summary
Abstract: Endoscopically assisted surgery has become an essential component in many fields of surgical specialties. The implementation of this technique to craniofacial and maxillofacial surgery is a recent development. Endoscopic approach to subcondylar mandible fractures has been established as reliable surgical method.

An audit on orthognathic surgery: a single surgeon’s experience
Journal of Craniofacial Surgery
Date: 2008
Doctor Author: Dr Vincent Yeow, Y C Por
Research Type: Retrospective clinical audit / single-surgeon case series
Treatment Area: Plastic and reconstructive surgery; craniofacial and orthognathic surgery; audit of orthognathic surgery outcomes and case mix
Publication Summary
Abstract:The aim of this article was to present a retrospective audit on a single surgeon’s experience with orthognathic surgery. This was a retrospective review of orthognathic cases performed from January 1, 2000, to January 1, 2006. There were 37 male and 65 female patients with a mean age of 20 years. Predisposing conditions included: unilateral cleft lip and palate (40), bilateral cleft lip and palate (15), cleft palate (three), hemifacial microsomia (three), posttraumatic (three), fibrous dysplasia (one), Romberg’s disease (one), cavernous hemangioma (one), Crouzon’s syndrome (one), and developmental deformities (34: 13 prognathism, 12 class III, six class II, three vertical maxillary excess). Indications for surgery included: class III malocclusion (89), class II malocclusion (six), facial asymmetry (three), vertical maxillary excess (three), crossbite (one). The majority of surgeries performed were Le Fort I osteotomy alone (33) and bimaxillary osteotomy (32). Overall median duration for all surgery was 2 hours 45 minutes (range, 1 hour 15 minutes to 8 hours 45 minutes), median blood loss was 720 mL (range, 100-6500 mL), and mean hospitalization stay was 4.3 days (range, 1-10 days). The mean duration of follow up was 24 months. Postoperatively, class I occlusion was obtained in 92 patients and class II occlusion in two patients. Relapse occurred in five (4.9%) patients (one had reoperation). Readjustment was done for three patients. Excessive bleeding occurred from the facial artery, maxillary artery, and pterygoid plexus separately in three patients. Readmission for secondary hemorrhage occurred twice and inferior alveolar nerve injury occurred once.
Platelet-rich plasma has no effect on increasing free fat graft survival in the nude mouse
Journal of Plastic, Reconstructive & Aesthetic Surgery
Date: 2009
Doctor Author: Yong-Chen Por, Dr Vincent Yeow, Nayef Louri, Tony Kiat-Hon Lim, Irene Kee, In-Chin Song
Research Type: Experimental animal study
Treatment Area: Plastic and reconstructive surgery; fat grafting; platelet-rich plasma and free fat graft survival
Publication Summary
Abstract:The aim of this article was to present a retrospective audit on a single surgeon’s experience with orthognathic surgery. This was a retrospective review of orthognathic cases performed from January 1, 2000, to January 1, 2006. There were 37 male and 65 female patients with a mean age of 20 years. Predisposing conditions included: unilateral cleft lip and palate (40), bilateral cleft lip and palate (15), cleft palate (three), hemifacial microsomia (three), posttraumatic (three), fibrous dysplasia (one), Romberg’s disease (one), cavernous hemangioma (one), Crouzon’s syndrome (one), and developmental deformities (34: 13 prognathism, 12 class III, six class II, three vertical maxillary excess). Indications for surgery included: class III malocclusion (89), class II malocclusion (six), facial asymmetry (three), vertical maxillary excess (three), crossbite (one). The majority of surgeries performed were Le Fort I osteotomy alone (33) and bimaxillary osteotomy (32). Overall median duration for all surgery was 2 hours 45 minutes (range, 1 hour 15 minutes to 8 hours 45 minutes), median blood loss was 720 mL (range, 100-6500 mL), and mean hospitalization stay was 4.3 days (range, 1-10 days). The mean duration of follow up was 24 months. Postoperatively, class I occlusion was obtained in 92 patients and class II occlusion in two patients. Relapse occurred in five (4.9%) patients (one had reoperation). Readjustment was done for three patients. Excessive bleeding occurred from the facial artery, maxillary artery, and pterygoid plexus separately in three patients. Readmission for secondary hemorrhage occurred twice and inferior alveolar nerve injury occurred once.
Use of tissue sealants in face-lifts: a metaanalysis
Aesthetic Plastic Surgery
Date: 2009
Doctor Author: Yong-Chen Por, Luming Shi, Miny Samuel, Colin Song, Dr Vincent Yeow
Research Type: Meta-analysis / systematic review of comparative clinical studies
Treatment Area: Aesthetic plastic surgery; face-lift surgery; use of tissue sealants to reduce postoperative drainage, ecchymosis, oedema and haematoma risk
Publication Summary
Methods: The electronic databases MEDLINE (1966-May 2007) and EMBASE (1974-May 2007) and the Cochrane Central Register of Controlled Trials (CENTRAL) were searched for human studies, randomized controlled trials, controlled clinical trials, metaanalyses, and reviews of randomized controlled trials using the key words “fibrin tissue adhesive,” “tissue sealant,” “platelet-rich plasma,” “face-lift,” “rhytidoplasty,” “rhytidectomy,” and “facial plastic surgery.” The search yielded 10 articles, only 3 of which met our inclusion criteria. The three studies were within-patient comparisons (patients acted as their own controls).
Results: Although not statistically significant, the pooled results showed a strong trend toward reduction in postoperative drainage at 24 h and ecchymosis with the use of tissue sealants compared with the control arm of the study. No difference in outcomes was observed between the tissue sealant and control arms of the study in terms of postoperative edema measurement.

A unique presentation of epignathus
Journal of Craniofacial Surgery
Date: 2010
Doctor Author: Janna Joethy, Yong Chen Por, Dr Vincent Yeow
Research Type: Case report / craniofacial surgical case study
Treatment Area: Plastic and reconstructive surgery; craniofacial surgery; epignathus and rare congenital oropharyngeal teratoma management
Publication Summary
Abstract: Palatal clefts in conjunction with space-occupying lesions of the oral or nasal cavities are of interest because they may represent a developmental etiology of palatal clefts. Epignathus is a rare space-occupying tumor of the nasopharynx that can arise from the upper jaw, palate, and sphenoid. It can protrude through the mouth, causing respiratory embarrassment and death. The pathogenesis of epignathus is unknown, but several theories have been proposed. Management depends on the size of the tumor and requires a multidisciplinary approach.
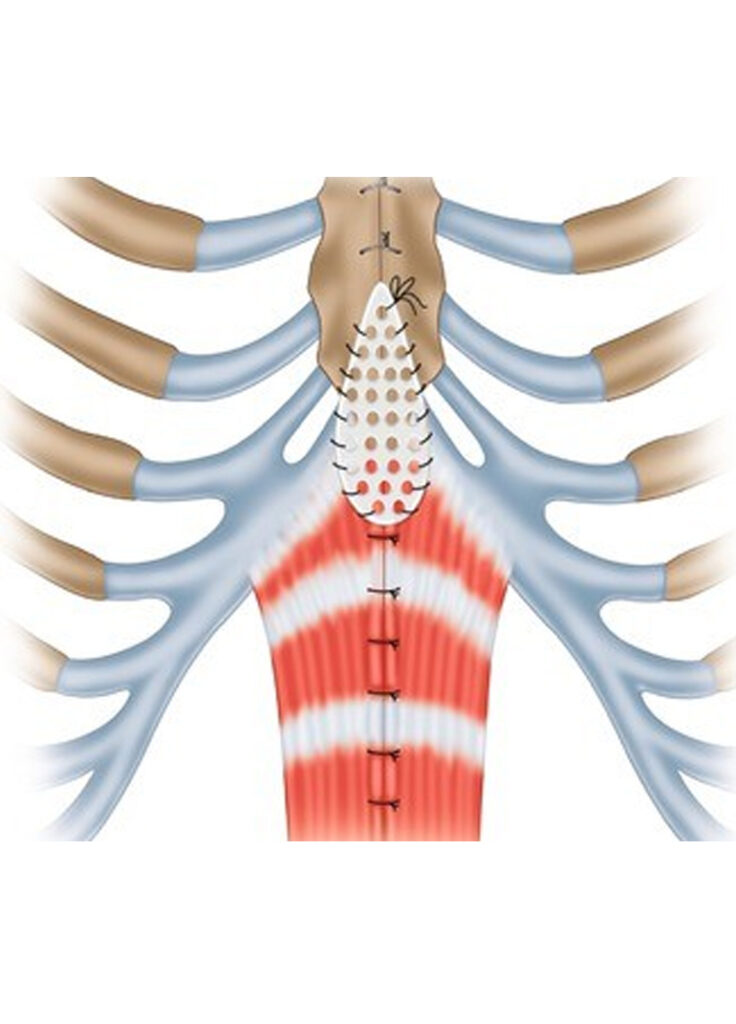
Journal of Pediatric Surgery
Date: 2012
Doctor Author: Hui-Ling Chia, Mohamed Zulfikar Rasheed, Kim-Kiat Ong, Dr Vincent Yeow
Research Type: Case report / paediatric reconstructive surgery technique article
Treatment Area: Plastic and reconstructive surgery; paediatric chest wall reconstruction; ectopia cordis repair in pentalogy of Cantrell using a resorbable poly-L-lactic-polyglycolic acid plate
Publication Summary
Abstract: We present a case of a 10-month-old male infant with thoracoabdominal ectopia cordis, as part of Cantrell pentad, repaired using a poly-L-lactic-polyglycolic acid plate, a resorbable plating system widely used in craniomaxillofacial reconstruction. This is the first reported case of sternal reconstruction using a poly-L-lactic-polyglycolic acid plate. The repair was successfully carried out without cardiopulmonary compromise and good aesthetic outcome was achieved.
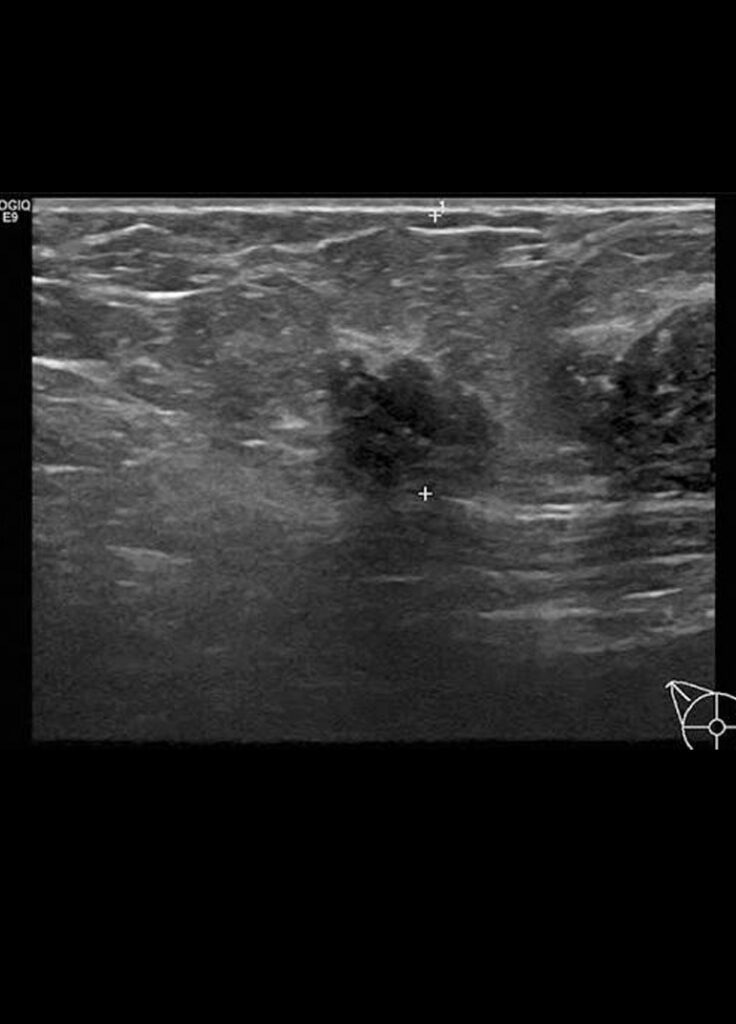
The use of microdebrider for the treatment of accessory axillary breast
Journal of Plastic, Reconstructive & Aesthetic Surgery
Date: 2012
Doctor Author: Sun Mingfa Jeremy, Chong Si Jack, Dr Vincent Yeow, Woo Kok Yen Evan
Research Type: Clinical technique article / minimally invasive surgical technique
Treatment Area: Plastic and reconstructive surgery; accessory axillary breast tissue; microdebrider-assisted excision for axillary contour correction
Publication Summary
Abstract: Accessory axillary breast tissue can be fairly common occurring in 2-6% of women. Treatment modalities thus far include direct excision as well as liposuction. While direct excision allows for accessible and adequate tissue resection, it results in long unsightly scars and the creation of significant amount of dead space. This may be complicated by seroma and haematoma formation. Liposuction is not without its drawbacks either. It is often very difficult to remove fibro-glandular breast tissue resulting in inadequate excision, thus leaving behind a visible core of breast tissue. This has led some surgeons to use a combination of direct excision and liposuction to manage accessory axillary breast tissue. Hence, we present the use of the microdebrider for sharp and precise excision of accessory axillary breast tissue. This day procedure can be performed through a single 5-mm incision which is well hidden in the axillary skin folds while allowing the operator the amount of control needed to accurately remove fibro-glandular breast tissue and restore an aesthetically pleasing contour to the axilla.
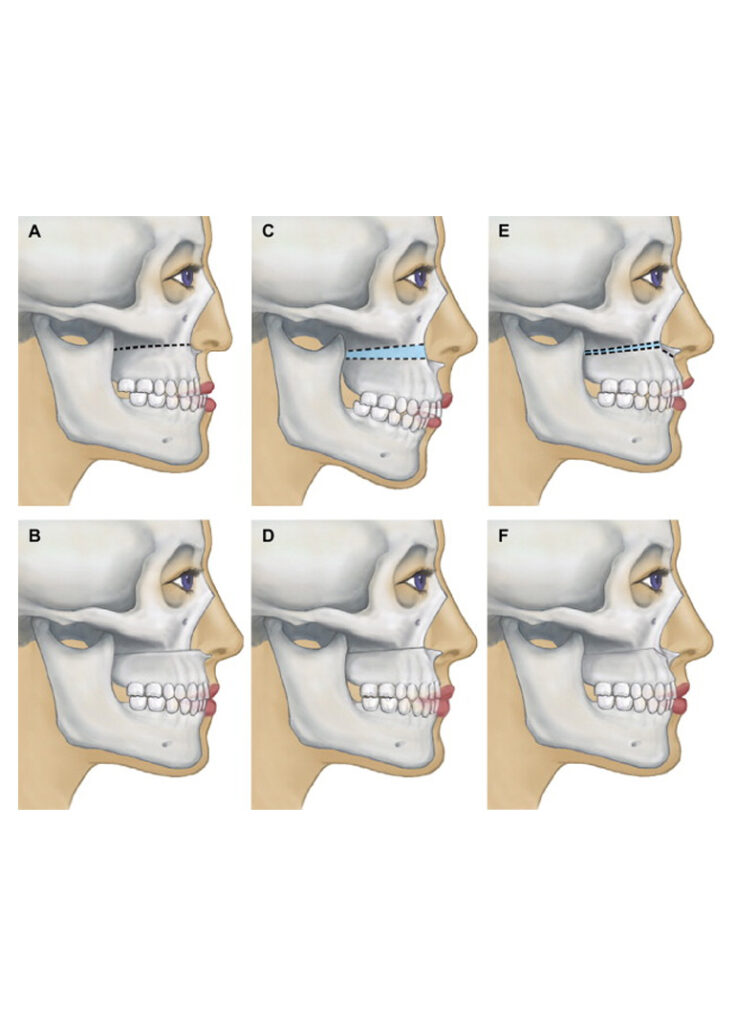
High Le Fort I and bilateral split sagittal osteotomy in Crouzon syndrome
Journal of Craniofacial Surgery
Date: 2013
Doctor Author: Yoong Chuan Tay, Kian Hian Tan, Dr Vincent Yeow
Research Type: Case report / craniofacial surgical case study
Treatment Area: Plastic and reconstructive surgery; craniofacial and orthognathic surgery; High Le Fort I and bilateral sagittal split osteotomy for Crouzon syndrome-related midface deficiency and jaw malocclusion
Publication Summary
Abstract: Crouzon syndrome is a rare, autosomal dominant disease from a fibroblast growth factor receptor 2 gene mutation, characterized by premature craniosynostosis, hypertelorism, orbital proptosis, psittichorina, hypoplastic maxilla, and mandibular prognathism. We present an adult 32-year-old Crouzon syndrome patient who underwent an elective High Le Fort I and bilateral split sagittal osteotomy for midface advancement with a background of jaw malocclusion and obstructive respiratory symptoms. The operation features a potential dynamic movement of the secured airway in the surgical field and close proximity to exposed ocular structures. Permissive hypotensive anesthesia was employed to improve the surgical field and reduce intraoperative blood loss and dose of long-acting opioids. He was extubated at the end of an uneventful surgery and was monitored in the high dependency overnight before he was discharged to the general ward. Perioperative issues include potential difficult airway management; ocular, auditory, and neurological injury prevention; surgery-specific anesthetic technique; and postoperative analgesia. Understanding the multisystemic issues facilitates the dynamic anesthetic management during surgery. Good communication among the multidisciplinary team is essential to ensure a successful operation and uneventful recovery.

Archives of Plastic Surgery
Date: 2014
Doctor Author: Hui-Ling Chia, Dr Vincent Yeow
Research Type: Case report / paediatric reconstructive surgical technique article
Treatment Area: Plastic and reconstructive surgery; paediatric chest wall reconstruction; inferior sternal cleft repair in pentalogy of Cantrell using bilateral sternal bar turnover flaps
Publication Summary
Abstract: We report a case of sternal reconstruction using bilateral sternal bar turnover flaps in a 4-year-old boy with an inferior sternal cleft, as part of Cantrell’s pentad. When the patient was 10 months old, he underwent sternal reconstruction using a resorbable poly-L-lactic-polyglycolic acid plate in the first stage when there was insufficient autogenous tissue to provide a reliable reconstruction. Bilateral sternal bar turnover was performed in the second stage at 4 years of age. This operative technique is described in this report. This novel technique provides a robust, dynamic, and reliable reconstruction for inferior sternal defects.

The Cleft Palate-Craniofacial Journal
Date: 2015
Doctor Author: Zhi Yang Ng, Selena Ee-Li Young, Yong Chen Por, Dr Vincent Yeow
Research Type: Retrospective clinical study
Treatment Area: Plastic and reconstructive surgery; cleft palate surgery; primary Furlow palatoplasty for submucous cleft palate in syndromic and nonsyndromic children
Publication Summary
Main outcome measures: Primary outcomes were based on postoperative perceptual speech assessments and the need for revision surgery. Secondary outcomes included improvement in nasalance scores, postoperative complications, and change in and time to normalization of velar closing ratios.
Results: Mean age at surgery = 7.7 years. Of the patients, 17 (50%) were syndromic and 11 (32%) had associated hearing loss. Mean follow-up = 48 months. No patients had postoperative complications, such as wound dehiscence or fistula; however, two patients (one syndromic, one nonsyndromic) required secondary procedures. Velar closing ratios for all patients increased (P < .05) and approached normal at an average of 1.3 years postoperatively.

Surgery-first orthognathic approach case series: salient features and guidelines
Journal of Orthodontic Science
Date: 2016
Doctor Author: Narayan H Gandedkar, Chai Kiat Chng, Winston Tan
Research Type: Case series / clinical guideline article
Treatment Area: Orthognathic surgery; surgery-first approach; treatment planning and clinical guidelines for dentofacial deformity correction
Publication Summary
Abstract: Conventional orthognathic surgery treatment involves a prolonged period of orthodontic treatment (pre- and post-surgery), making the total treatment period of 3-4 years too exhaustive. Surgery-first orthognathic approach (SFOA) sees orthognathic surgery being carried out first, followed by orthodontic treatment to align the teeth and occlusion. Following orthognathic surgery, a period of rapid metabolic activity within tissues ensues is known as the regional acceleratory phenomenon (RAP). By performing surgery first, RAP can be harnessed to facilitate efficient orthodontic treatment. This phenomenon is believed to be a key factor in the notable reduction in treatment duration using SFOA. This article presents two cases treated with SFOA with emphasis on “case selection, treatment strategy, merits, and limitations” of SFOA. Further, salient features comparison of “conventional orthognathic surgery” and “SFOA” with an overview of author’s SFOA treatment protocol is enumerated.

Surgery-first orthognathic approach case series: salient features and guidelines
Journal of Orthodontic Science
Date: 2016
Doctor Author: Narayan H Gandedkar, Chai Kiat Chng, Winston Tan
Research Type: Case series / clinical guideline article
Treatment Area: Orthognathic surgery; surgery-first approach; treatment planning and clinical guidelines for dentofacial deformity correction
Publication Summary
Abstract: Conventional orthognathic surgery treatment involves a prolonged period of orthodontic treatment (pre- and post-surgery), making the total treatment period of 3-4 years too exhaustive. Surgery-first orthognathic approach (SFOA) sees orthognathic surgery being carried out first, followed by orthodontic treatment to align the teeth and occlusion. Following orthognathic surgery, a period of rapid metabolic activity within tissues ensues is known as the regional acceleratory phenomenon (RAP). By performing surgery first, RAP can be harnessed to facilitate efficient orthodontic treatment. This phenomenon is believed to be a key factor in the notable reduction in treatment duration using SFOA. This article presents two cases treated with SFOA with emphasis on “case selection, treatment strategy, merits, and limitations” of SFOA. Further, salient features comparison of “conventional orthognathic surgery” and “SFOA” with an overview of author’s SFOA treatment protocol is enumerated.
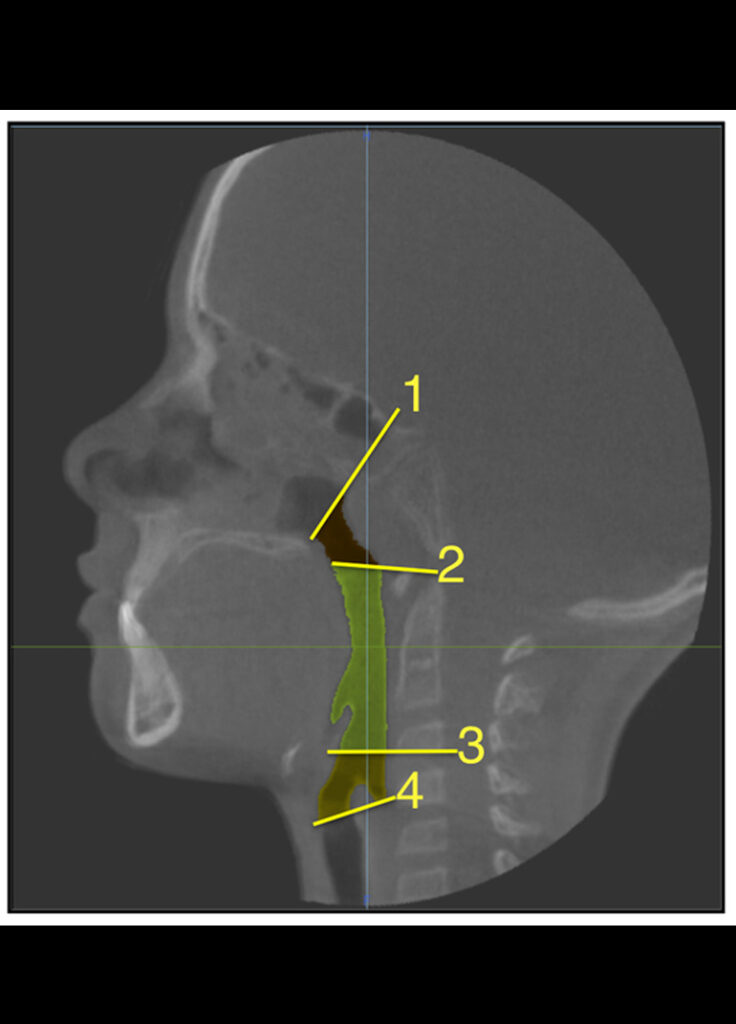
The Cleft Palate-Craniofacial Journal
Date: 2017
Doctor Author: Narayan H. Gandedkar, Chai Kiat Chng, Mohammed Asif Basheer, Peter Y. Chen, Dr Vincent Yeow
Research Type: Retrospective cone beam computed tomography study
Treatment Area: Plastic and reconstructive surgery; cleft lip and palate; pharyngeal airway space assessment in unilateral and bilateral cleft patients
Publication Summary
Materials and methods: Twenty UCLP (mean age: 13.4 ± 0.5 years), 18 BCLP (mean age: 13.5 ± 0.5 years) and 20 skeletal Class I subjects (mean age: 13.4 ± 0.6 years) were included in the study. Cone beam computed tomography scans were assessed for pharyngeal airway space (PAS) (oropharyngeal, nasopharyngeal, total airway space volume), and compared with PAS of age and sex-matched skeletal Class I NC individuals.
Results: Pharyngeal airway space showed statistically significant differences in the UCLP, BCLP, and NC control subjects. Oropharyngeal (9338 ± 1108 mm3, P < .05), nasopharyngeal (2911 ± 401 mm3, P < .05), and total airway space (12 250 ± 1185 mm3, P < .05) volumes of BCLP individuals showed significant reduction in comparison to UCLP and NC. There were no gender differences of PAS in any of the groups tested (P > .05).
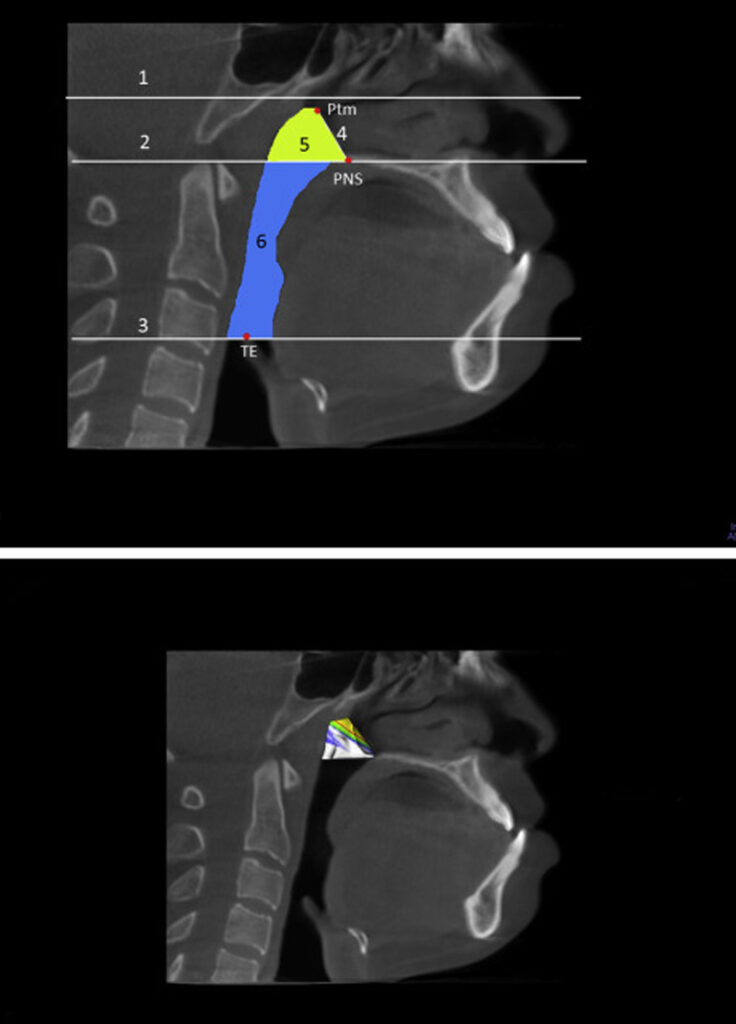
Journal of Oral and Maxillofacial Surgery
Date: 2017
Doctor Author: Narayan H. Gandedkar, Chai Kiat Chng, Yong Chen Por, Dr Vincent Yeow, Andrew Tjin Chiew Ow, Tian Ee Seah
Research Type: Clinical study / cone-beam computed tomography and questionnaire-based airway assessment
Treatment Area: Orthognathic surgery; Class III dentofacial deformity; pharyngeal airway changes and sleep apnoea assessment after bimaxillary surgery
Publication Summary
Patients and methods: This retrospective cohort study was composed of patients with skeletal Class III discrepancy who underwent bimaxillary jaw surgery and were assessed with STOP-BANG score, cephalometry, and cone-beam computed tomography (of the PAS). The predictor variable was bimaxillary jaw surgery and included 4-, 6-, and 8-mm setbacks. The primary outcome variables were PAS volume, body mass index, and STOP-BANG score evaluated at 1 week before surgery and after comprehensive orthodontic treatment (11.25 ± 1.95 months). Other variables were grouped into the following categories: demographic and cephalometric parameters. Statistical intragroup and intergroup differences were assessed by paired t and independent t tests (P < .05), respectively.
Results: The study sample was composed of 48 patients (18 to 25 yr old); group I received 4-mm setback (n = 16), group II received 6-mm setback (n = 16), and group III received 8-mm setback (n = 16) mandibular surgery, and all test groups received 4-mm maxillary advancement. The entire study group was compared with a skeletal Class I control group (n = 16). The total PAS volume after orthodontic treatment in groups I and II showed a significant decrease compared with the presurgical PAS (P < .001), but the decrease was not less than that in the control group (P > .05). In contrast, the total PAS volume in group III after orthodontic treatment (23,574 ± 1,394 mm3) was less than that in the control group (23,884 ± 1,543 mm3).
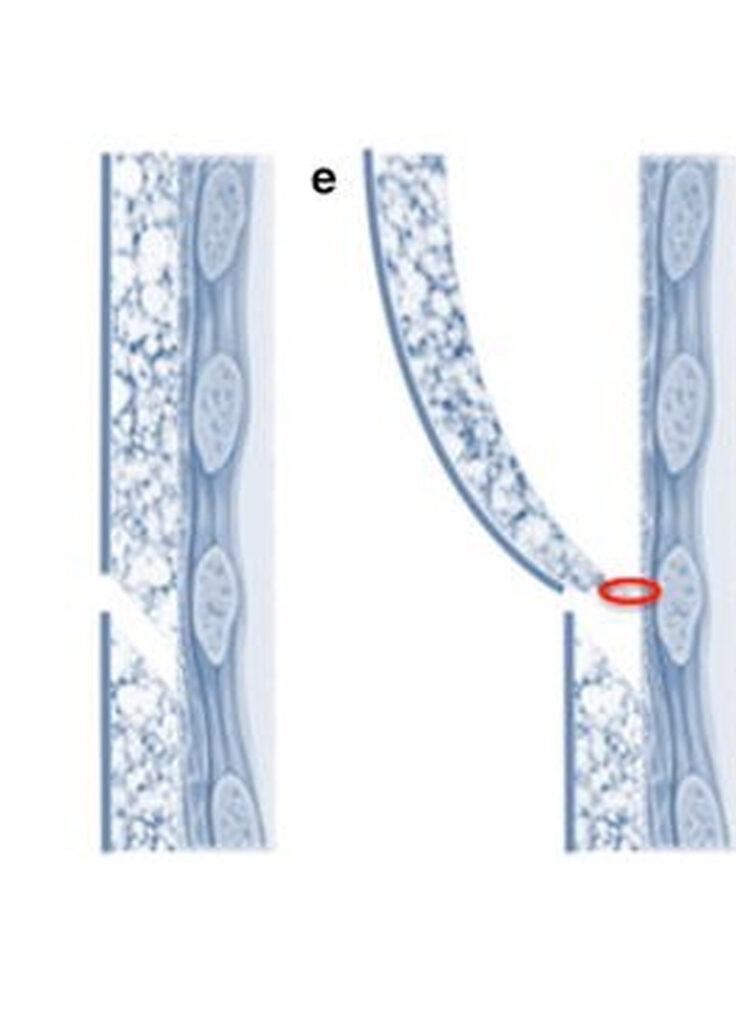
Archives of Plastic Surgery
Date: 2018
Doctor Author: Charles Randquist, Yong Chen Por, Dr Vincent Yeow, Jan Melchizedek Maglambayan, Susan Simonyi
Research Type: Retrospective chart review / patient-reported outcomes study
Treatment Area: Aesthetic plastic surgery; breast augmentation; inframammary fold incision and patient-reported outcomes in Southeast Asian women
Publication Summary
Methods: Through a retrospective chart review, patients who underwent primary breast augmentation with anatomical form-stable silicone gel breast implants using an inframammary fold incision were followed for ≥6 months postoperatively. The BREAST-Q Augmentation Module (scores standardized to 0 [worst] – 100 [best]) and Patient and Observer Scar Assessment Scale (POSAS; 1 [normal skin] to 10 [worst scar imaginable]) were administered. Responses were summarized using descriptive statistics. Patient-reported events were collected.
Results: Twenty-two Southeast Asian patients (mean age, 35.1 years) completed ≥1 postoperative BREAST-Q and POSAS assessment and were assessed 11 months to 5.5 years postoperatively. The mean postoperative BREAST-Q satisfaction with breasts and psychosocial well-being scores were 69.2 and 84.0, respectively. The mean POSAS score for their overall opinion of the scar was 4.2; the mean scores for all scar characteristics ranged from 1.2 to 4.2. Over 90% of patients (20/22) said that they would recommend the procedure. Patient complaints following surgery included anisomastia (possibly pre-existing; n=2), sensory loss at the nipple (n=2) or around the nipple (n=3), scarring (n=4), and slight capsular contracture (n=1). No patients required reoperation.

Determinants of Planned Orthognathic Surgical Movements in a Singaporean Cleft Lip and Palate Cohort
Journal of Craniofacial Surgery
Date: 2026
Doctor Author: Boon Hui Chan, Aik Wei Goh, Chieh Shen Koo, Chai Kiat Chng, Dr Vincent Yeow, Yong Chen Por
Research Type: Retrospective cohort study
Treatment Area: Plastic and reconstructive surgery; cleft lip and palate; orthognathic surgical planning and determinants of planned surgical movements in cleft patients
Publication Summary
Abstract: Cleft lip and palate are frequently associated with disturbances in maxillary growth, and many patients require orthognathic surgery at skeletal maturity. This study aimed to characterize baseline craniofacial morphology and determine factors influencing the magnitude of planned orthognathic surgical movements in a Singaporean cleft cohort managed using virtual surgical planning (VSP). A retrospective cohort study was conducted, including non-syndromic cleft patients who underwent orthognathic surgery between 2020 and 2025 at a tertiary cleft center in Singapore. All procedures were planned using VSP and performed with customized cutting guides and fixation plates. Demographic variables, preoperative cephalometric parameters (SNA, SNB), and planned skeletal and dental movements were extracted from surgical planning records. Forty-four patients were included (20 males, 24 females). The median age at surgery was 20.24 years (IQR 19.67-22.46). Male patients underwent surgery at a significantly older age than females (22.21 versus 19.87 y, P < 0.001) and demonstrated greater baseline maxillary retrusion (median SNA 73.05 degrees versus 77.50 degrees, P = 0.007). Planned maxillary advancement was significantly greater in males for both A-point (8.18 ± 2.19 mm versus 5.88 ± 2.05 mm; P < 0.001) and maxillary incisor tip movement (7.55 ± 1.94 mm versus 5.25 ± 2.24 mm, P < 0.001). SNB differed significantly across cleft subtypes (P = 0.005), although the magnitude of planned surgical movements did not differ significantly between cleft phenotypes. These findings suggest that while sex and cleft phenotype influence baseline craniofacial morphology, planned orthognathic surgical movements remain broadly comparable across cleft subtypes within contemporary VSP workflows.