



Temple Acne Scar Removal Using Subcision: Scaffolding Support With Sutures and Collagen‑Stimulating Fillers
Temple acne scars are frequently perceived as stubborn because they tend to combine two difficult features: the scar is often physically tethered beneath the skin, and the temple region itself can show contour deficiency or hollowing that amplifies shadowing. In practice, this means a temple scar may remain visible even after surface‑level interventions, such as topical agents or mild resurfacing, because the primary problem is not only pigment or texture but also the mechanical pull of fibrous bands and the loss of supportive volume.
For this reason, contemporary “temple acne scar treatment using subcision” is often discussed as a structured, multimodal strategy rather than a single procedure. The central idea is to address the scar’s tethering first, then stabilise the released space so that the tissue does not collapse or re‑adhere, and finally support longer‑term collagen remodelling.
Subcutaneous incisionless surgery, commonly known as subcision and frequently misspelled online as “subscision,” is a well‑established technique designed to release the fibrotic attachments that pull atrophic scars downward. A comprehensive review of subcision for atrophic acne scars describes subcision as a minimally invasive procedure in which an instrument is introduced to detach scars adhering to the underlying subcutaneous layer, with subsequent wound healing responses contributing to connective tissue growth and contour improvement.
In a temple‑focused context, doctors sometimes extend this concept further by introducing an internal support step, which patients may hear described as “scaffolding.” In practical terms, “temple scaffolding acne scar treatment” refers to the deliberate creation of internal support after subcision, such as a suture‑based traction or thread support concept, frequently complemented by a collagen‑stimulating filler such as Ellansé or Radiesse.
Why temple acne scars require a tailored strategy
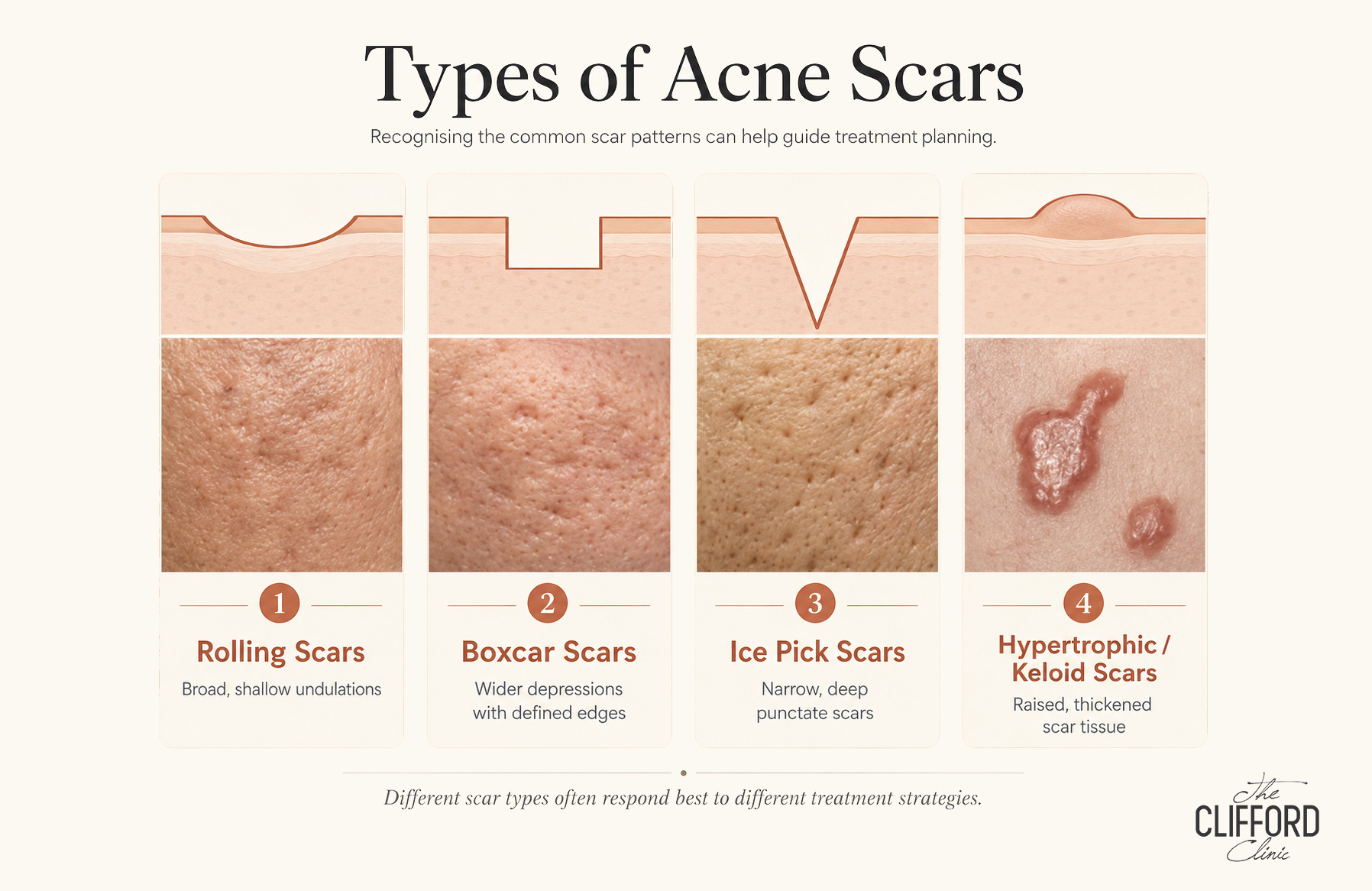
Atrophic acne scars are typically categorised into rolling, boxcar, and ice‑pick morphologies, and they frequently coexist in the same patient. The subcision literature emphasises that scar morphology matters because it determines which interventions are most likely to succeed. In the temple, rolling and tethered boxcar patterns are often clinically relevant because these forms of scarring can involve fibrous strands at the dermal‑subcutaneous junction that pull the skin downward. The same comprehensive subcision review explains that subcision is effective precisely because it physically disrupts those fibrotic attachments, allowing the surface to lift as the dermis detaches and as connective tissue fills the space during healing.
However, even when tethering is released, the temple may continue to show a depression due to limited soft tissue coverage and the natural curvature of the region. This is one reason why a purely surface‑oriented approach may not satisfy patients who primarily notice shadowing, dents, or contour irregularity in side lighting. When the objective is to minimise a visible depression at the temple, the plan often needs to address both tethering and structural support.
Subcision in formal terms: what it targets and why it works
Subcision is best understood as a procedure aimed at the mechanical cause of certain depressed scars. In atrophic scarring, fibrous bands can attach the dermis to deeper tissues, and these attachments create a persistent downward pull.
In a CNA Brand Spotlight feature, Dr Gerard Ee is quoted explaining that over‑the‑counter creams are typically insufficient for depressed scars because meaningful improvement requires replacing damaged dermal collagen structures, and that treatment selection differs by scar type. While that article focuses on device‑based modalities, the principle is the same: a depressed scar is, fundamentally, a structural problem.
Because subcision creates a subdermal pocket or plane where the adhesions were released, clinicians often consider whether the released area will heal in an elevated position or whether it will collapse or re‑adhere. This is where “scaffolding” becomes clinically relevant.
What “scaffolding” means after subcision in the temple area
“Scaffolding” refers to an internal support concept that helps stabilise the tissue after scar release. Once adhesions are disrupted, the tissue has an opportunity to remodel, but remodelling occurs over time. The earliest healing period is therefore critical, because re‑tethering or collapse can reduce the durability of improvement.
One illustrative example is the open‑access study “Treatment of Skin Depression with Combined Upward Suture Traction and Percutaneous Subcision,” which evaluated a technique for soft‑tissue depressions and retracted scars. In that report, the authors describe placing a looping suture at the core of the depression to provide vertical traction and facilitate release of adhesions via percutaneous subcision, and they report that bruising persisted for two to three weeks in treated areas, with other outcomes varying by site. Although this study is not specific to acne scars at the temple, it provides a peer‑reviewed demonstration of the broader principle that suture traction can be used as an internal support manoeuvre in combination with subcision when the goal is to correct a depression.
The acne scar literature also supports the general idea that combining subcision with supportive adjuncts can improve clinical outcomes. A PubMed‑indexed study evaluating subcision alone versus subcision combined with cross‑linked hyaluronic acid or threads in atrophic post‑acne scars found higher rates of significant clinical improvement in the combined groups than in the subcision‑only group, with reported side effects described as tolerable and transient within the study’s context. Again, while this study is not limited to temple scars, it supports the rationale that an internal support or augmentation component can strengthen the overall result when scar tethering is only one part of the problem.
Why collagen‑stimulating fillers are often used as part of the support strategy
Dermal fillers are widely discussed as a component of multimodal acne scar management, particularly for atrophic rolling and boxcar scars where soft‑tissue augmentation can elevate depressions. A review focusing on fillers for acne scar improvement explains that fillers can be categorised as temporary, semipermanent, or permanent, and it notes that semipermanent or biostimulatory fillers such as calcium hydroxylapatite can provide stronger collagen stimulation than some temporary options. The same review also stresses that safety and tolerability depend on filler properties, practitioner skill, anatomical knowledge, and patient factors, and it explicitly states that fillers should not be used in children and youngsters, underscoring the importance of age‑appropriate clinical decision‑making.
In the context described by the user, two collagen‑stimulating fillers are commonly cited in aesthetic practice: Ellansé, which is PCL‑based, and Radiesse, which is CaHA‑based. Although clinical practices vary and regulatory approvals differ by jurisdiction, the shared rationale is that these products may provide structural support while also encouraging longer‑term collagen remodelling.
Ellansé as a collagen stimulator used for structural support
Ellansé is described in its Summary of Safety and Clinical Performance as a PCL‑based injectable implant intended for subdermal implantation in the face for correction of wrinkles and facial aging signs or conditions. From a mechanistic standpoint, the published clinical literature describes PCL‑based fillers as providing immediate volume due to a carrier gel component while supporting longer‑term volumising effects through collagen stimulation associated with PCL microspheres. A paper assessing the long‑term volumising action of a PCL‑based filler reports sustained volumising effects of at least two years in the cases studied and interprets the increase in volume beyond the injected amount as indicative of neocollagenesis induced by PCL microspheres.
When this concept is translated into “temple acne scar treatment using subcision,” Ellansé is sometimes discussed as part of a plan that combines scar release, internal stabilisation, and longer‑term collagen rebuilding.
Radiesse as a collagen‑stimulating filler with formal safety information
Radiesse is a CaHA‑based dermal filler that has FDA approvals for certain indications. An FDA Summary of Safety and Effectiveness Data document for Radiesse (+) Lidocaine states that the product is indicated for subdermal implantation for correction of moderate to severe facial wrinkles and folds such as nasolabial folds, and it also includes an indication for improving moderate to severe loss of jawline contour in adults.
In scientific and clinical narrative reviews, CaHA microspheres are described as a scaffold that can stimulate fibroblast activity and promote neocollagenesis, which supports the common description of Radiesse as both a volumiser and a biostimulatory agent. This is the conceptual basis for its inclusion as a “collagen stimulating filler” in some acne scar strategies, particularly when longer‑term tissue quality and structural support are part of the therapeutic objective.
What patients commonly experience after subcision and supportive interventions
Subcision and related supportive techniques can involve visible but temporary downtime, most commonly bruising and swelling. In the study combining upward suture traction with percutaneous subcision, bruising persisted for two to three weeks around treated areas, and induration persisted longer in some cases. In the acne‑scar‑specific study comparing subcision alone versus combinations with hyaluronic acid or threads, the authors describe side effects as tolerable and transient in the context of the study design and follow‑up. While individual experience varies, these descriptions provide a reasonable basis for understanding that bruising and short‑term tissue firmness can occur and should be anticipated.
When fillers are included, the safety information provided by manufacturers and regulators should be part of the discussion, including the rare but serious risk of unintentional intravascular injection and the more common local adverse events. In a temple‑based plan, it is also reasonable for patients to ask about the clinician’s anatomical approach, the rationale for product selection, and the clinic’s readiness to identify and manage complications.
FAQ
Is the temple a higher‑risk area for injectable treatments?
Yes. The temple region is considered anatomically complex, and although serious complications are uncommon, medical literature has specifically investigated the risk of vision loss associated with temple filler injections and discussed potential vascular pathways linking temporal arteries to the ophthalmic circulation. For this reason, any plan involving injections in the temple—particularly with non‑reversible or biostimulatory materials—should be approached conservatively and performed only by appropriately trained medical professionals with strong anatomical expertise.
What side effects or downtime can occur after subcision‑based procedures?
Temporary bruising, swelling, and tenderness are common after subcision.
How many sessions are typically needed, and when do results become visible?
The number of sessions depends on scar type, severity, and whether the plan includes combination modalities such as threads, fillers, or resurfacing. In general, subcision aims to release tethering immediately, but visible improvement often continues to evolve as collagen remodeling progresses over time, which is part of the rationale for collagen‑stimulating materials that demonstrate sustained volumizing and tissue effects in published studies. Because treatment response is highly individualized, a responsible clinical plan is typically staged and adjusted based on healing and interval improvement rather than promised as a one‑session transformation.
Conclusion
Temple acne scars can be particularly conspicuous because the region’s contour and lighting sensitivity amplify depressions, and because the scar itself may be tethered beneath the skin. In such cases, temple acne scar treatment using subcision can be a rational starting point because subcision directly targets the fibrous attachments that pull the scar downward and can stimulate connective tissue growth during healing.
The notion of “scaffolding” adds a second layer of rationale: once tethering is released, internal support may help stabilise the tissue while remodelling occurs, and published techniques combining suture traction with subcision demonstrate how traction can be integrated to treat depressions. Acne scar studies also suggest that combining subcision with threads or augmentation can produce better outcomes than subcision alone in selected settings.
When collagen‑stimulating fillers such as Ellansé (PCL) or Radiesse (CaHA) are discussed as part of this approach, the underlying objective is to provide structural support and encourage longer‑term collagen remodelling, while recognising that these devices are subject to specific indications, safety information, and age considerations. Because the temple is a higher‑risk anatomical area and rare but severe vascular complications have been investigated in the scientific literature, any such plan must be framed as a specialist medical intervention, not a routine cosmetic add‑on.
References
- Vempati A, Zhou H, Hession MT, et al. “Subcision for Atrophic Acne Scarring: A Comprehensive Review of Surgical Instruments and Combinatorial Treatments.” Published in 2023 and available via PubMed Central.
- Ebrahim HM, Nassar A, ElKashishy K, et al. “A combined approach of subcision with either cross-linked hyaluronic acid or threads in the treatment of atrophic acne scars.” PubMed record and abstract.
- Pereira OJ, Bins-Ely J, Ferreira LM. “Treatment of Skin Depression with Combined Upward Suture Traction and Percutaneous Subcision.” Published in 2015 and available via PubMed Central.
- Wollina U. “Fillers for the improvement in acne scars.” Published in 2015 and available via PubMed Central.
- Angelo‑Khattar M, Casabona G, et al. “Objective Assessment of the Long‑Term Volumizing Action of a Polycaprolactone‑Based Filler.” Published in 2022 and available via PubMed Central.
- U.S. Food and Drug Administration. “Summary of Safety and Effectiveness Data (SSED) for RADIESSE® (+) Lidocaine injectable implant.” Includes indications and the adult over 21 language for jawline contour indication.
- Sheth NT, Hauck MJ, et al. “Risk of Blindness From Temple Filler Injections: Investigating Vascular Anastomoses Between the Deep Temporal and Ophthalmic Arteries.” PubMed record and abstract.
- Frontiers in Surgery. “Leveraging anatomy to improve safety and efficacy in temple augmentations—a case series of 20 patients.” Discussion of temporal anatomy complexity and risk considerations by injection plane.
- ScienceDirect (Elsevier). “An illustrated anatomical approach to reducing vascular risk during facial soft tissue filler administration – a review.” General discussion of vascular complication risk and the need for depth‑aware anatomy.