



Role of Baby Skin Booster in Korean Glass skin
Why “repair mode” matters for skin quality
Why “repair mode” matters for skin quality. Many skin concerns that people label as “ageing” or “bad skin” are, biologically, variations of the same theme: the skin is behaving as if it is still repairing an injury. When that state becomes persistent, skin can look dull, uneven, reactive and less resilient.
Texture becomes less refined, pores look more obvious and fine lines can appear earlier than expected. In some individuals, acne, dermatitis, friction, repeated device irritation, or chronic sun exposure keeps the skin in a cycle of low-grade inflammation that never fully resolves. The key players behind this pattern are cytokines (immune signalling proteins) and matrix metalloproteinases (MMPs) (enzymes that break down parts of the extracellular matrix).
When cytokines remain elevated for too long, they continue to drive MMP activity. Over time, this can prevent stable remodelling and contribute to a skin environment that is constantly rebuilding and degrading at the same time.
This article explains, from a medical perspective, how this cycle works and where an ECM-focused approach such as Re2O skin booster protocols, may fit into a broader skin-quality plan.
A short framework: healing vs remodelling vs scarring
Skin repair is not a single event. It is a coordinated sequence that generally moves through phases: an initial response to limit damage, an inflammatory phase to clear debris and recruit repair cells, a proliferative phase where new matrix and vessels form and a remodelling phase where the structure matures and strengthens.
The difference between an ideal outcome and a disappointing one is often not “did healing happen,” but “what type of tissue formed.” In constructive remodelling, the repaired tissue becomes more organised and functional. In a scar-dominant outcome, the structure can be more chaotic, mechanically different and less efficient.
Even when there is no visible “scar,” a chronic repair-state can still lead to micro-level disorganisation in the dermis that shows up as uneven texture, reduced elasticity and a persistently “tired” surface appearance.
A major determinant of which direction the skin takes is the quality of the extracellular matrix (ECM) present during healing. The ECM is not just a passive scaffold. It is an active biological structure that stores signals, binds cytokines and growth factors and provides mechanical and biochemical cues that influence how cells behave.
What the ECM actually does
The extracellular matrix is the three-dimensional network around skin cells. It contains structural proteins (such as collagen), glycoproteins, proteoglycans and glycosaminoglycans. Clinically, you can think of it as the skin’s “support environment”: it anchors cells, supports hydration handling, provides mechanical resilience and acts as a communication platform that helps cells decide whether to migrate, proliferate, produce collagen, or settle down.
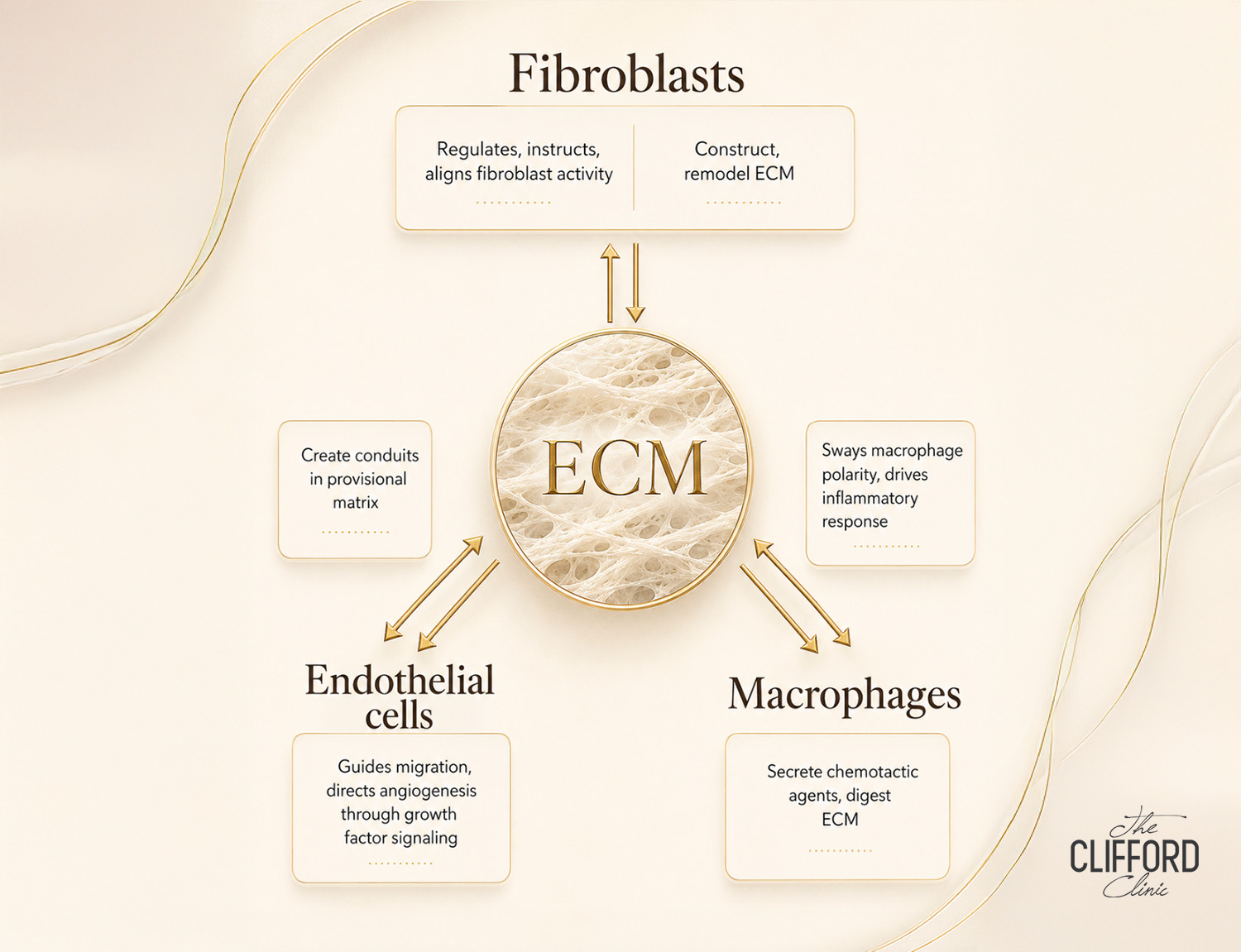
A useful concept is dynamic reciprocity, the ongoing two-way interaction between cells (such as fibroblasts, endothelial cells and immune cells like macrophages) and the ECM. Cells remodel the matrix; the matrix then influences what those cells do next. When the matrix is healthy, these interactions help the skin return to balance after stress. When the matrix is damaged or disorganised, the signalling environment becomes distorted and inflammation can persist.
Cytokines: the signals that can either resolve inflammation or prolong it
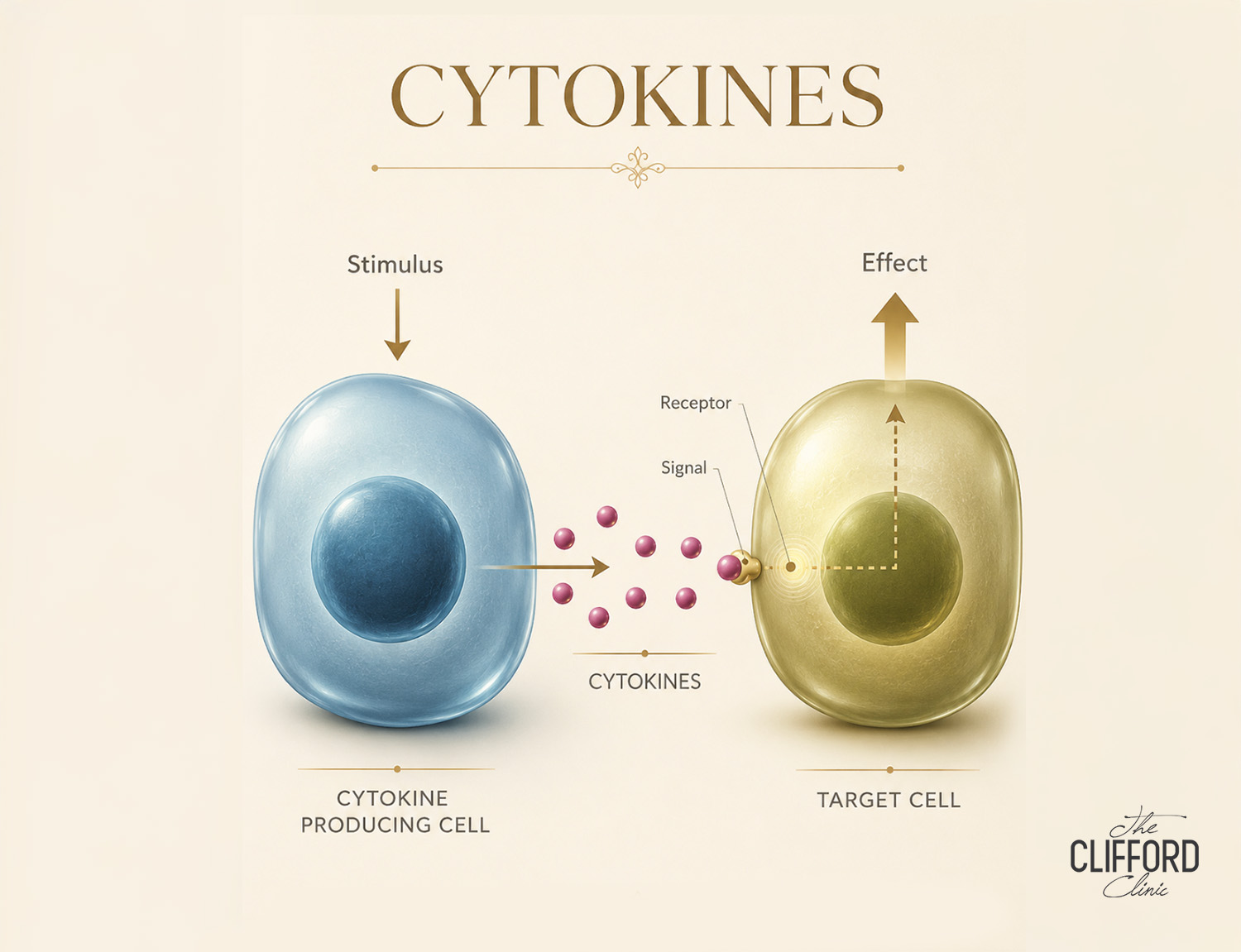
Cytokines are messenger proteins released by immune cells, skin cells and vascular cells. Some cytokines promote inflammation and recruit more immune cells. Others help switch inflammation off and support rebuilding.
In acute injury, cytokines are useful. They coordinate early clean-up, recruit cells that rebuild tissue and activate pathways that restore function. Problems arise when the cytokine profile stays skewed toward a pro-inflammatory state. In that scenario, the skin can remain “on alert,” repeatedly triggering a wound-like program even when the trigger is minor or already resolved.
In aesthetic practice, common triggers that can keep cytokines elevated include persistent acne inflammation, barrier disruption from over-exfoliation, chronic UV exposure, repeated friction or picking and untreated inflammatory dermatoses. In Singapore, additional contributors can include high UV exposure, heat and sweating that aggravate acne/folliculitis in some patients and alternating humidity with air-conditioned dryness that destabilises barrier function in others.
MMPs: why the matrix keeps getting broken down
Matrix metalloproteinases (MMPs) are enzymes that degrade components of the ECM. They are not inherently harmful. Controlled MMP activity is necessary for normal remodelling: old or damaged matrix must be broken down so new matrix can be laid down in an organised way.
The issue is excessive or prolonged MMP activity, particularly when driven by ongoing inflammatory cytokines. When MMP levels remain high, the skin’s supportive matrix is continuously fragmented. Fibroblasts then struggle to build durable, well-aligned collagen because the environment they are building into is unstable.
This is one reason why some skin looks as if it is never quite “finishing” recovery: the construction site keeps getting disrupted.
Clinically, MMP-driven matrix breakdown is relevant not only to chronic wounds, but also to chronic inflammatory skin states and photoageing. UV exposure is known to upregulate MMP pathways and contribute to collagen fragmentation over time. In inflammatory acne, local cytokines and protease activity can contribute to tissue breakdown that predisposes to atrophic scarring in susceptible individuals.
Why some skin gets “stuck”: the chronic inflammation pattern
When skin remains in a chronic inflammatory state, a typical pattern appears: persistently elevated pro-inflammatory cytokines, increased protease activity (including MMPs) and comparatively reduced availability of signals that support orderly closure and stable remodelling. In this setting, the inflammatory phase of repair does not transition cleanly into a mature remodelling phase.
Fibroblast function becomes less efficient, angiogenesis and nutrient delivery can be less coordinated and the matrix becomes more degraded and disorganised.
This “stuck” pattern explains why some patients describe cycles of temporary improvement followed by relapse, especially with barrier-damaging routines or repeated irritation. The skin may look better briefly when swelling or hydration increases but it does not consolidate into improved structure because the underlying signalling environment remains dominated by inflammation and matrix breakdown.
The ECM as a cytokine regulator (not just a scaffold)
A clinically important point is that ECM is not neutral with respect to cytokines. Many ECM macromolecules have binding sites that capture cytokines and growth factors, influencing their local concentration, half-life and activity. A healthy ECM can help shape the local immune environment toward resolution and rebuilding.
When the ECM is damaged, those binding interactions can be lost or altered. This can contribute to a more chaotic cytokine environment and allow chronic inflammation to persist.
In practical terms, if the matrix cannot “hold” and organise signalling molecules properly, the tissue may struggle to progress to a stable outcome.
This concept is one reason ECM-focused materials have been used in other fields to support constructive tissue remodelling. While aesthetic injectables are not the same as surgical graft materials, the biological principle remains clinically relevant: improving the matrix environment can change how cells behave during recovery.
“Cytokine reservoir”: why matrix-bound signals matter
Another useful concept is that ECM can act as a reservoir of latent bioactivity. Growth factors and cytokines can be stored bound to matrix proteins and released in a controlled way as the matrix is remodelled.
This is different from adding a single molecule into tissue and hoping it diffuses to the right place. Matrix-bound signalling can be more spatially organised and can persist long enough to influence later phases of remodelling.
From a medical planning standpoint, this helps explain why “more inflammation” does not equal “more collagen,” and why controlled, guided remodelling tends to produce more consistent texture outcomes than repeated cycles of irritation.
Mechanobiology: how mechanical forces shape inflammation and scarring
Skin is a mechanical organ. Fibroblasts respond to the stiffness and organisation of the matrix around them. When tissue is exposed to abnormal mechanical cues such as excess stiffness, disorganised fibres, or persistent tension, fibroblasts may shift toward a more contractile phenotype associated with scar-like remodelling. Mechanical cues also interact with inflammatory pathways, which means that tissue mechanics can influence cytokine profiles and vice versa.
In aesthetic terms, this is one reason why some areas (such as the jawline or perioral region) can develop stubborn texture issues: mechanical stress and repeated micro-inflammation can reinforce each other.
A treatment plan that aims to improve skin quality should therefore consider not only “stimulation,” but whether the tissue environment supports organised remodelling rather than prolonged repair signalling.
Where a “Re2O skin booster” fits into this model
Re2O skin booster is commonly positioned as an ECM-based skin booster, often described as using micronised human acellular dermal matrix (hADM) components rather than being a purely hyaluronic-acid hydration product. The clinical rationale behind ECM-oriented injectables is not simply to add volume or water, but to support the dermal micro-environment where remodelling occurs.
In the context of inflammation, the intent is typically to work with (not against) biology:
-
Reduce the likelihood of prolonged repair signalling by avoiding overly aggressive stacking and by supporting barrier stability.
-
Support collagen remodelling in a way that is compatible with the skin’s recovery capacity.
-
Improve overall skin behaviour (texture, resilience and recovery consistency) rather than chasing short-lived changes.
It is important to state this conservatively: clinical outcomes vary. Results depend on the specific injectable used, technique, dosing, patient factors and whether the baseline inflammatory state has been addressed.
Who tends to benefit most from an inflammation-aware plan
Patients who often benefit from an inflammation-aware approach (rather than simply adding more procedures) include those with:
Skin that flushes easily, stings with many products, or reacts unpredictably; persistent acne-related inflammation even when breakouts are mild; texture that looks uneven despite good hydration; early loss of elasticity with a dull surface; or post-inflammatory changes that linger after minor irritation.
These patterns do not always mean a diagnosed skin disease, but they suggest the local environment may be skewed toward ongoing immune signalling and matrix breakdown. In such cases, procedures that repeatedly inflame the skin without a stabilising plan can lead to slow or inconsistent gains.
A Re2O collagen booster plan generally works best when combined with barrier repair, trigger control and appropriate device selection.

What treatment typically involves
Most Re2O skin booster protocols are delivered as a series, with spacing determined by the clinician based on skin behaviour, tolerance and goals. Treatment is typically performed with topical anaesthesia when appropriate, using small deposits distributed across targeted zones.
Aftercare generally focuses on minimising unnecessary irritation, reducing heat exposure for a short period and monitoring for bruising or swelling.
Because technique matters, outcomes can vary. In inflammation-prone patients, conservative dosing, careful spacing and avoiding multiple inflammatory procedures too close together usually improves tolerability.
Safety and side effects
As with other injectable skin boosters, the expected short-term effects of Re2O skin booster include redness, swelling, tenderness and bruising. Small bumps can occur depending on technique and typically settle as swelling resolves and the product integrates.
Less common risks include infection, prolonged inflammation, hypersensitivity reactions and vascular complications if a product is inadvertently placed within a vessel. Informed consent should include warning symptoms and a clear follow-up plan.
Patients with active skin infection, uncontrolled inflammatory dermatoses, or certain medical conditions may be advised to defer treatment until stabilised.
How to avoid staying “stuck” after procedures
Inflammation should be purposeful and time-limited. If a procedure repeatedly creates flare-ups that last beyond the expected recovery window, the plan may need adjustment. Barrier function should be stabilised before and after procedures, especially in patients using retinoids, exfoliating acids, or acne treatments that increase sensitivity.
Trigger control, such as UV protection, acne management, friction avoidance and treatment spacing, often makes more difference than adding another procedure.
Mechanistically, the goal is to move skin from a state dominated by pro-inflammatory cytokines and excessive protease activity toward a state where fibroblasts can rebuild a more organised matrix and then exit “repair mode.”
Combining Re2O collagen booster with other treatments
In practice, Re2O skin booster protocols work best when they are placed inside a clear treatment architecture, rather than “added on” after a procedure, because the skin still looks tired. The reason is biological. Most energy-based devices and many injectable programmes create a controlled injury.
That controlled injury can be useful when the goal is remodelling but if it is layered too aggressively or layered onto already inflamed, barrier-compromised skin, the net effect can shift from constructive remodelling to prolonged irritation. The skin then behaves as if it needs to keep repairing, which is the opposite of what you want when you are aiming for stable texture, calmer tone and better elasticity.
If pigment and uneven tone are the dominant issues, it is usually more appropriate to control pigment drivers and reduce ongoing triggers first, then use injectables to support skin quality and recovery. For a pigment-focused pathway, see: pigmentation removal treatment.
If the main issue is active acne, sequence matters even more. Procedures that increase inflammation on top of uncontrolled inflammatory acne can prolong redness, increase sensitivity and raise the risk of post-inflammatory marks. In acne-prone patients, the medically sensible order is usually: first control active lesions and inflammation, then address texture and dermal quality. Once acne activity is stabilised, Re2O may be considered as part of the recovery and skin-quality phase, particularly if the skin has lingering roughness, reduced resilience, or slow “bounce-back” after breakouts. For the acne pathway, see: acne treatment Singapore.
If active acne is present, sequence matters. Treat acne activity and inflammation first, then address texture and dermal quality. For more information, refer to: HIFU non-surgical face lifting.
If collagen rebuilding and structural refinement are priorities, Re2O collagen booster may be planned alongside collagen-stimulating injectables (bioregenerative fillers), with deliberate spacing and clear goals for each layer (skin quality vs structural support). For collagen-stimulating options, see: collagen bioregenerative filler Singapore.
A simple way to interpret sequencing is: you want skin to progress from repair mode → remodelling mode → maintenance mode. Stacking too many inflammatory triggers too close together keeps resetting the cycle back to repair mode.
Frequently Asked Questions on Re2O Skin Booster Singapore
Is Re2O mainly for hydration?
Re2O skin booster is typically discussed as an ECM-focused skin booster rather than a purely hydration-focused HA booster. Patients may still notice improved glow and comfort, but the clinical positioning is usually centred on supporting skin quality and dermal resilience rather than short-term “water plumpness” alone.
How soon do results appear?
Some patients notice early improvements in surface hydration and texture within days to weeks, while changes associated with remodelling are usually assessed over a longer period. Clinically, it is reasonable to evaluate response after completing a planned series rather than judging after one session.
Will it help if my skin is inflamed or acne-prone?
It depends on the type and control of inflammation. Active inflammatory acne or dermatitis usually needs primary medical management first. Once inflammation is controlled, a skin booster plan may support recovery and texture goals. If inflammation remains active, adding procedures can sometimes worsen reactivity.
Can it be combined with Thermage or HIFU?
Combination planning is common in aesthetic practice, but timing and sequencing should be individualised. The goal is to avoid excessive overlapping inflammation while supporting longer-term structural improvements.
Where The Clifford Clinic fits in
At The Clifford Clinic, Re2O skin boosters are offered as part of a structured skin-quality programme rather than a one-size-fits-all injection schedule. Consultation focuses on identifying what is keeping the skin in a persistent repair-state, ongoing inflammation, barrier instability, pigment drivers, acne activity, mechanical stress, or a combination, so the plan supports stable remodelling rather than short-lived change.
Closing clinical takeaway
When skin remains “stuck” in repair mode, it is often because inflammatory signalling persists and MMP activity continues to break down the extracellular matrix, so the dermis cannot transition into orderly, stable remodelling. In that setting, repeated stimulation without a coherent plan can add more inflammatory load and further delay recovery. A more durable approach is to treat the ECM as an active regulator of skin behaviour: it binds and organises signalling molecules, modulates bioactivity over time and provides mechanical cues that influence how fibroblasts and immune cells respond.
Within this framework, Re2O skin booster Singapore protocols are commonly used as an ECM-focused option to support the dermal environment where recovery and remodelling take place, alongside barrier optimisation, trigger control and careful sequencing with devices or other injectables. The Clifford Clinic offers Re2O as part of a structured skin-quality programme, where the treatment plan is built around skin assessment and recovery dynamics rather than a one-size-fits-all injection schedule.
References
- Hodde JP, Hiles MC. The Interplay of ECM-Based Graft Materials and Mechanisms of Tissue Remodeling. In: Extracellular Matrix – Developments and Therapeutics. IntechOpen; 2021. doi:10.5772/intechopen.96954.
- Schultz GS, Davidson JM, Kirsner RS, Bornstein P, Herman IM. Dynamic reciprocity in the wound microenvironment. Wound Repair Regen. 2011;19:134–148. doi:10.1111/j.1524-475X.2011.00673.x.
- Eming SA, Martin P, Tomic-Canic M. Wound repair and regeneration: mechanisms, signaling and translation. Sci Transl Med. 2014;6:265sr6.
- Gurtner GC, Werner S, Barrandon Y, Longaker MT. Wound repair and regeneration. Nature. 2008;453:314–321. doi:10.1038/nature07039.
- Lazaro JL, Izzo V, Meaume S, Davies AH, Lobmann R, Uccioli L. Elevated levels of matrix metalloproteinases and chronic wound healing: an updated review of clinical evidence. J Wound Care. 2016;25:277–287. doi:10.12968/jowc.2016.25.5.277.
- Quan T, Qin Z, Xia W, Shao Y, Voorhees JJ, Fisher GJ. Matrix-degrading metalloproteinases in photoaging. J Investig Dermatol Symp Proc. 2009;14:20–24.
- Wynn TA, Vannella KM. Macrophages in tissue repair, regeneration and fibrosis. Immunity. 2016;44:450–462.
- Xu R, Boudreau A, Bissell MJ. Tissue architecture and function: dynamic reciprocity via extra- and intra-cellular matrices. Cancer Metastasis Rev. 2009;28:167–176. doi:10.1007/s10555-008-9178-z.
- Bissell MJ, Hall HG, Parry G. How does the extracellular matrix direct gene expression? J Theor Biol. 1982;99:31–68.
- Kular JK, Basu S, Sharma RI. The extracellular matrix: structure, composition, age-related differences, tools for analysis and applications for tissue engineering. J Tissue Eng. 2014;5:2041731414557112. doi:10.1177/2041731414557112.
- Sun WQ, Xu H, Sandor M, Lombardi J. Process-induced extracellular matrix alterations affect the mechanisms of soft tissue repair and regeneration. J Tissue Eng. 2013;4:2041731413505305. doi:10.1177/2041731413505305.
- Badylak SF. The extracellular matrix as a biologic scaffold material. Biomaterials. 2007;28:3587–3593. doi:10.1016/j.biomaterials.2007.04.043.