



An evidence based guide to knee pain, meniscus damage, cartilage damage, ACL and PCL injury and the best PRP injection for knee joint
People often search for the best knee joint injection doctor and the best knee joint injection clinic because knee pain interrupts work, sport, sleep and daily life. The choice of doctor and clinic matters. An accurate diagnosis matters together with the product and technique of the injection matters. The follow up rehabilitation matters too. This guide explains how to choose wisely in Singapore, how different injections work and how published research supports your decision, including the work co-authored by Dr Gerard Ee and how this has influenced how surgeons and sports doctors think about knees.
What a top knee injection service does differently
A service that deserves to be called the best knee joint injection clinic will do three things very well. It will give you a precise diagnosis. It will match the injection to that diagnosis and to your goals. It will track outcomes and adjust the plan.
A precise diagnosis separates common pathways of knee pain. Osteoarthritis is not the same as a focal cartilage lesion. Meniscus tears behave differently from tendon overload or bursitis. Cruciate ligament injury creates instability and swelling that follow their own pattern. A thoughtful service explains what is driving your pain and what the knee injections are trying to achieve. That reduces the risk of doing the right treatment for the wrong problem.
Technique and product matter. It follows evidence for dosing and spacing of injections. It sequences care. That may mean a short acting steroid for an inflamed flare, a cycle of hyaluronic acid for mechanical lubrication, or platelet rich plasma for a longer horizon of symptom control and function.
Measurable outcomes should result in a significant improvement in pain and function scores, strength testing, range of motion and patient specific goals. When the plan works, you will see the numbers move in the right direction.
Why the doctor’s research pedigree still matters in 2025
You want a clinician who reads the science and contributes to it. Dr Gerard Ee is an example of that profile. He co-authored a prospective study in The Knee that used computer navigation during total knee replacement to measure the joint line in real time. The study found that patients whose joint line moved by four millimetres or more had worse outcome scores, while careful measurement helped surgeons avoid those larger deviations. That sounds technical. In practice it reflects a habit of precision with small details that affect results in real life.
He also co-authored an editorial that challenged the vague label patellofemoral syndrome. The idea is simple. A catch all label is not a diagnosis. A precise description of what is wrong under the kneecap leads to more targeted and effective care. That mindset improves decisions about injections because it pushes the team to treat the driver of pain rather than the symptom alone.
These publications build reputation because they show a pattern. Accurate diagnosis leads to the correct treatment. Link technical accuracy through proper imaging techniques with either X-rays or MRI and this leads to better patient reported outcomes. Those are the habits you want in the person who chooses and delivers your injection.
The main intra articular injection options explained
Corticosteroid
This is an anti-inflammatory injection that can settle a hot and swollen knee. Relief is often quick and can help you start or restart exercise therapy. Most guidelines describe its benefit as short term. Over use is discouraged. It works best when the goal is to calm a flare while you address load and strength.
Hyaluronic acid
This is a lubricant like gel that aims to improve the glide inside an arthritic joint. Evidence is mixed across guidelines. Some groups recommend it in selected patients. Others are more cautious and conditionally recommend against routine use for knee osteoarthritis. Many patients still report meaningful relief. Benefit appears greater in mild to moderate disease and when paired with activity change and strength work.
Platelet rich plasma
This is prepared from your own blood and concentrates platelets and plasma proteins. It aims to modulate inflammation and support joint homeostasis. A large network meta analysis published in 2024 compared common intra articular injections across forty eight trials and more than nine thousand knees with at least six months of follow-up. Platelet-rich plasma had the highest probability of improving pain and function at six months or longer. Bone marrow aspirate concentrate and hyaluronic acid ranked behind platelet rich plasma, while steroids ranked lowest over that time horizon.
Bone marrow aspirate concentrate
This is a concentrate of your own bone marrow that contains a mixture of cells and growth factors. Evidence is smaller than for platelet-rich plasma and hyaluronic acid, but promising studies report improved pain and function in osteoarthritis. Availability varies by clinic, and the conversation should include regulatory status and cost.
Effective PRP injection for knee joint. Formulation and protocol.
Patients often ask for the most effective PRP injection for knee joint problems. The honest answer is that details matter. Doctors prepare platelet-rich plasma with different centrifuge settings and with different white blood cell content. Some meta-analyses suggest that leukocyte-poor preparations may be linked with better pain outcomes for osteoarthritis and fewer post-injection reactions, but results are not entirely consistent across studies. What is consistent is that PRP as a category, outperforms placebo and often outperforms hyaluronic acid on pain and function across six to twelve months when high-quality trials are pooled. Your doctor should explain the preparation they use, why they prefer it and how many injections are planned.
A careful clinic will also set expectations. Some people feel a temporary ache for a day or two. Many protocols advise simple activity for forty-eight hours and a graded return to strength and gait work after that. Program design matters. The shot starts a process. Your training builds on it.
Choosing the best knee joint injection doctor in Singapore
Use four filters.
- First, look at diagnosis. Does the doctor take time to separate osteoarthritis from focal cartilage damage, meniscus injury, tendinopathy, bursitis, or a loose body. Do they use ultrasound or MRI when needed. Do they explain the pain source in plain language.
- Second, ask about technique. What approach is used. What volume and concentration. What is the plan if a flare occurs.
- Third, ask about evidence. Does the doctor quote high level reviews when comparing options. The 2024 network meta-analysis is a good benchmark when you discuss osteoarthritis. So are current guidelines on short term steroid benefit and the mixed stance on hyaluronic acid.
- Fourth, ask how success will be measured. Pain and function scores are a good start. Strength, range, and specific return to activity goals are even better. This is where the research focus on measuring what matters becomes visible in clinic life.
When knee joint injections are used for specific problems
Knee osteoarthritis and chronic knee pain
The main goals are pain relief, better function and easier exercise. Steroid can settle a flare over weeks. Hyaluronic acid can provide lubrication for months in selected patients. Platelet rich plasma is the front runner for six to twelve month improvement in many pooled trials. Bone marrow aspirate concentrate is an option in some clinics and has encouraging mid term follow up data. Your doctor will position these options within a full program that includes weight bearing strength, gait work, and load management.
Meniscus damage
Degenerative meniscus tears are common in middle age. Many improve with exercise therapy, education and load changes. When pain persists, a growing body of research explores platelet rich plasma. A 2024 systematic review of nonoperative platelet rich plasma for degenerative tears reported variable but generally favourable clinical outcomes and signal of structural benefit on MRI in some studies. When the tear is repaired surgically, augmentation with platelet rich plasma during the operation may reduce failure rates. Conversation with your doctor should cover tear type, age, activity goals and whether injection is stand alone or part of an operative plan.
Hyaluronic acid has been studied after arthroscopy and in meniscal pain with mixed results. Some reviews do not support a clear benefit after arthroscopy itself. Selected patients still report symptom relief when hyaluronic acid is used as a lubricant while they build strength. This again highlights the value of an individual plan rather than a single recipe.
Cartilage damage
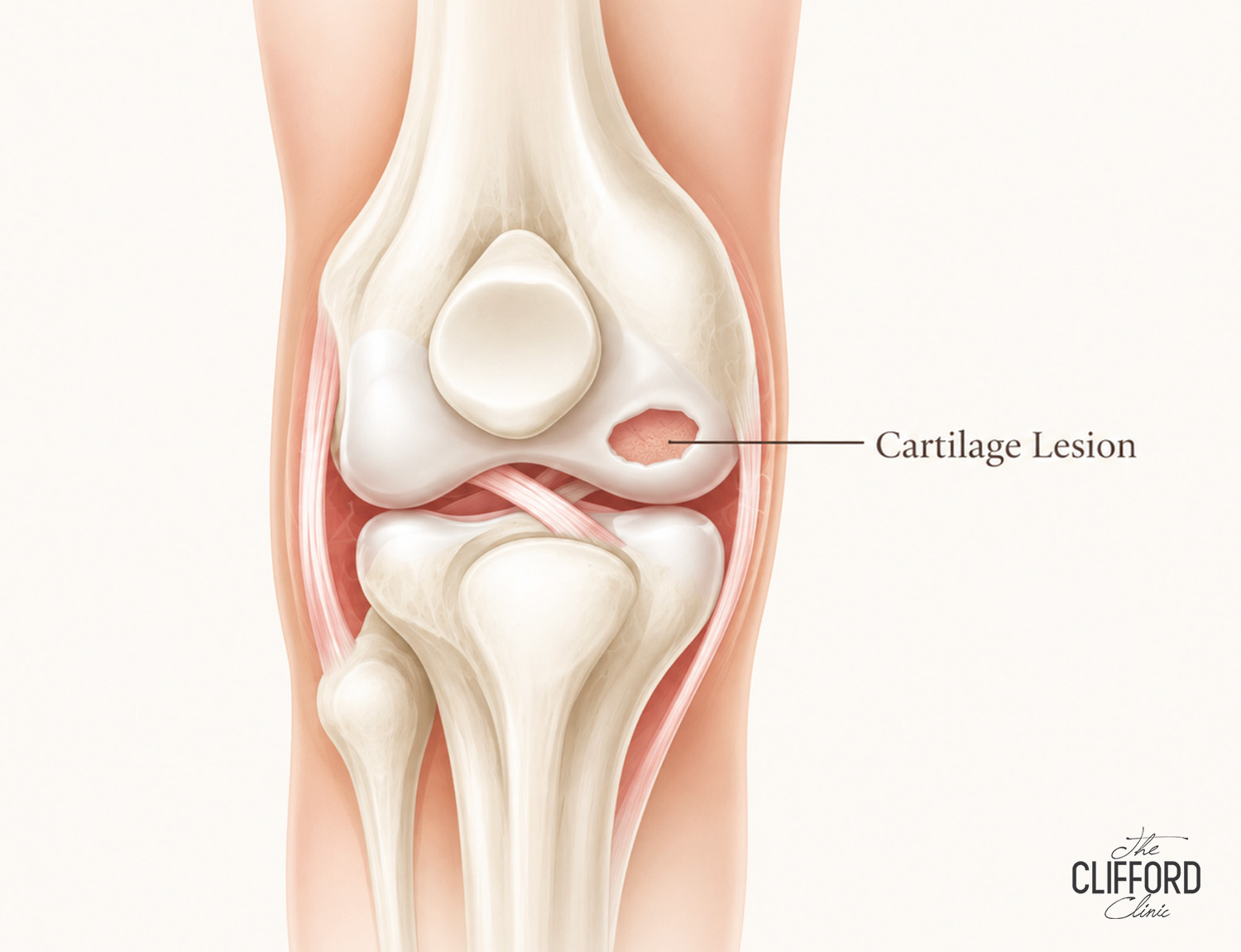
Focal cartilage lesions and early osteoarthritis are different problems. Cartilage defects can cause sharp pain with load in a specific zone, catching or swelling after sport. Several reviews discuss nonsurgical and surgical options, including injection strategies as supportive therapy. Platelet rich plasma has shown clinical improvement in many osteoarthritis trials and is often used to reduce symptoms around a focal lesion while a structured program progresses. Bone marrow aspirate concentrate is under active study and may improve pain and function in osteoarthritis across years of follow up. If a defect is large, surgery to restore the surface may be advised and adjuvant injections can support recovery in selected cases. A doctor who treats many cartilage problems will help you navigate these choices.
ACL and PCL injury
Cruciate ligament injuries produce swelling, instability and loss of confidence in pivoting movements. The role of injections is less settled than in osteoarthritis. In patients who undergo anterior cruciate ligament reconstruction, a well designed randomized trial in 2024 found that a single postoperative intra articular platelet rich plasma injection did not improve symptoms or function at twelve months. Other meta analyses show small or inconsistent advantages in stability or early pain and range, which do not always persist. For partial ACL tears and for nonoperative PCL injuries, biologic injections including platelet rich plasma have been explored in small studies and clinical series with promising signs. If you consider an injection for a cruciate injury, do so within a structured program that focuses on strength, neuromuscular control and return to sport criteria.
Knee inflammation and synovitis
Inflammation inside the knee joint can come from crystal disease, autoimmune arthritis, or an arthritic flare. Corticosteroid injection can be a helpful tool for short term control, especially when swelling and night pain limit sleep and exercise. Most guidelines recommend steroid as a short-term option with a plan to transition to exercise and disease specific care as the inflammation settles.
Building a reputation on measurable care. A note on Dr Gerard Ee
Patients often ask who is the best knee joint injection doctor. Rankings are subjective. What you can measure is the clinician’s approach to precision and outcomes. Dr Gerard Ee’s publications tell a useful story. The 2013 study in The Knee measured how small changes in joint line position after knee replacement correlate with patient reported outcomes. The team used computer navigation as an intra operative measuring tool and reported worse scores when the joint line changed by four millimetres or more. That is a tangible example of linking a technical detail with how a knee feels and functions in daily life. The 2009 editorial urged the field to avoid vague labels like patellofemoral syndrome and to get to the specific cause. Those two themes support trustworthy injection practice. Measure what matters. Name the real problem and treat it directly.

A practical pathway for people who want the best PRP injection for knee joint pain
Step one is a precise diagnosis. Confirm whether you are dealing with osteoarthritis, a focal cartilage lesion, a meniscus issue, or a ligament problem. If you have osteoarthritis and your goal is six to twelve months of improved pain and function while you keep moving, platelet rich plasma is a strong candidate based on the 2024 network meta analysis. Discuss the formulation that your clinic uses and the number of injections planned. Ask about short term activity advice after the shot and how to plug into strength and gait work during the response window.
If you have a degenerative meniscus tear and symptoms persist despite exercise therapy, platelet rich plasma can be considered as a targeted nonoperative option. If you need a surgical repair, talk about whether augmentation during the operation is planned and what that means for risk of re tear and recovery time. Approach hyaluronic acid as a lubricant option that can help selected patients. If you plan to return to sport after a cruciate injury, place injections in a supportive role rather than a primary fix unless high quality evidence shows otherwise for your specific scenario.
Finally, ask how success will be measured. Agree on baseline and follow up scores. Set a plan for next steps if targets are not met. The best knee joint injection clinic will welcome those questions and will have a clear system for answering them.
Frequently asked questions
How quickly will I feel better after a steroid, hyaluronic acid, or platelet rich plasma injection?
Steroid often calms a flare within days and the effect usually lasts weeks. Hyaluronic acid can take days to weeks to settle and often lasts months. Platelet rich plasma can take a few weeks to reach maximum benefit and often sustains improvement for six to twelve months in osteoarthritis. Individual response varies and your doctor can frame likely timelines for your case.
Is platelet rich plasma better than hyaluronic acid?
Across pooled randomized trials with at least six months of follow up, platelet rich plasma tends to outperform hyaluronic acid on pain and function. That does not mean every person will do better with platelet rich plasma. It does mean that it deserves serious consideration when the goal is a mid-term improvement without surgery.
Which PRP is best?
Many clinics prefer leukocyte poor preparations for osteoarthritis based on subgroup findings that suggest better pain outcomes and fewer flares. Other reviews find little difference between formulations. The most important factor is a clinician who understands their protocol and explains the rationale.
Can injections delay surgery?
Yes. Many patients use a sequence of injections and targeted strength training to stay active and to delay or avoid surgery. If arthritis advances and surgery becomes the right choice, modern knee replacement pays close attention to restoring the natural joint line. That principle is linked to better outcomes in published work and reflects the same focus on measurement that drives good injection practice.
How do I judge the best knee joint injection doctor?
Look for a precise diagnosis, image guided technique when appropriate, transparent use of evidence, and a plan to measure outcomes. Look for a doctor who explains what the injection is supposed to change and how you will know it worked.
The bottom line for knee joint injection Singapore
You get the best results when the right person receives the right injection for the right reason. For osteoarthritis, platelet rich plasma has strong pooled evidence for six to twelve month gains. Hyaluronic acid can help selected patients, and steroids are useful for short term flare control. Meniscus and cartilage problems require a careful blend of exercise therapy, load management, and targeted injections, with surgery considered when mechanics demand it. Cruciate ligament injuries sit at the edge of current injection evidence and deserve a cautious and individualized plan. Choose a doctor and clinic that value measurement and clarity. Published work by Dr Gerard Ee illustrates that habit of precision and outcome focus. That is what you want behind every injection you receive.
References
- Jawanda H, Khan ZA, Warrier AA, Acuña AJ, Allahabadi S, Kaplan DJ, et al. Platelet rich plasma, bone marrow aspirate concentrate, and hyaluronic acid injections outperform corticosteroids in pain and function scores at a minimum of six months as intra articular injections for knee osteoarthritis. A systematic review and network meta analysis. Arthroscopy. 2024 May. 40. 1623 to 1636. PubMed
- Ee G, Pang HN, Chong HC, Tan MH, Lo NN, Yeo SJ. Computer navigation is a useful intra operative tool for joint line measurement in total knee arthroplasty. Knee. 2013 Aug. 20. 256 to 262. PubMed
- Grelsamer R, Moss G, Ee G, Donell ST. The patellofemoral syndrome. The same problem as the Loch Ness Monster. Knee. 2009 Oct. 16. 301 to 302. PubMed
- Gopinatth V, Sullivan D, Muench LN, Frank RM, Yanke AB, Cole BJ. Degenerative meniscus tears treated nonoperatively with platelet rich plasma. A systematic review. Arthroscopy Sports Medicine and Rehabilitation. 2024. PMC
- Utrilla GS, Lamo Espinosa JM, Mora G, et al. Efficacy of platelet rich plasma in meniscal repair surgery. Systematic review and meta analysis. 2024. PubMed
- Ye Z, Jin S, Yang H, et al. Intra articular platelet rich plasma after anterior cruciate ligament reconstruction and patient outcomes at twelve months. Randomized clinical trial. JAMA Network Open. 2024. PMC
- Li G, Wang X, Zhang Y, et al. The effect of platelet rich plasma on clinical outcomes after anterior cruciate ligament reconstruction. Systematic review and meta analysis. 2025. PMC
- Bannuru RR, Osani MC, Vaysbrot EE, et al. OARSI guideline for the non surgical management of knee osteoarthritis. Osteoarthritis and Cartilage. 2019. PubMed
- Kolasinski SL, Neogi T, Hochberg MC, et al. 2019 American College of Rheumatology and Arthritis Foundation guideline for the management of osteoarthritis of the hand hip and knee. Arthritis Care and Research. 2020. PubMed
- Brittberg M. Treatment of knee cartilage lesions in 2024. From hyaluronic acid to regenerative medicine. Journal of Experimental Orthopaedics. 2024. PMC
- Pabinger C, Resch H, Frohner B, et al. Intra articular bone marrow aspirate concentrate injections for knee osteoarthritis. Four year follow up. Scientific Reports. 2024. Nature
- Glinkowski WM, Narloch J, Tomaszewski P. Intra articular hyaluronic acid for knee osteoarthritis. Review of current practice. Journal of Clinical Medicine. 2025. PMC
- Xiong Y, He J, Zhang Y, et al. Efficacy and safety of platelet rich plasma injections for knee osteoarthritis. A systematic review and meta analysis with subgroup analysis of leukocyte content. Frontiers in Medicine. 2023. Frontiers
- Gothesen O, Espehaug B, Havelin LI, et al. Computerized navigation as a useful tool in total knee replacement. A review of purpose and outcomes. 2020.