



How ECM Skinboosters Work
Written by Dr Law Zhi Wei
Most patients considering a skin booster treatment in Singapore want to know one thing above all else: how does this actually work? It is a fair question and an increasingly important one as the injectable category has expanded into ever-more-sophisticated formulations. ECM skinboosters, and Elravie Re2O in particular, represent a meaningful step beyond what was possible even a few years ago. Understanding why requires looking past the marketing language and examining what is actually happening at the cellular and molecular level when the product is injected into your skin.
This article is a clinical deep-dive into the mechanism of action behind Elravie Re2O. It is written for patients who want a sophisticated understanding of what they are receiving, and for clinicians who want to understand why this category genuinely warrants the attention it has been receiving across Korean and increasingly global aesthetic medicine. By the end, you will understand not just what an ECM skinbooster does but why it does what it does, and why the science behind it represents a categorical shift rather than an incremental improvement.
Starting With the Cell: Fibroblasts as the Architects of Skin
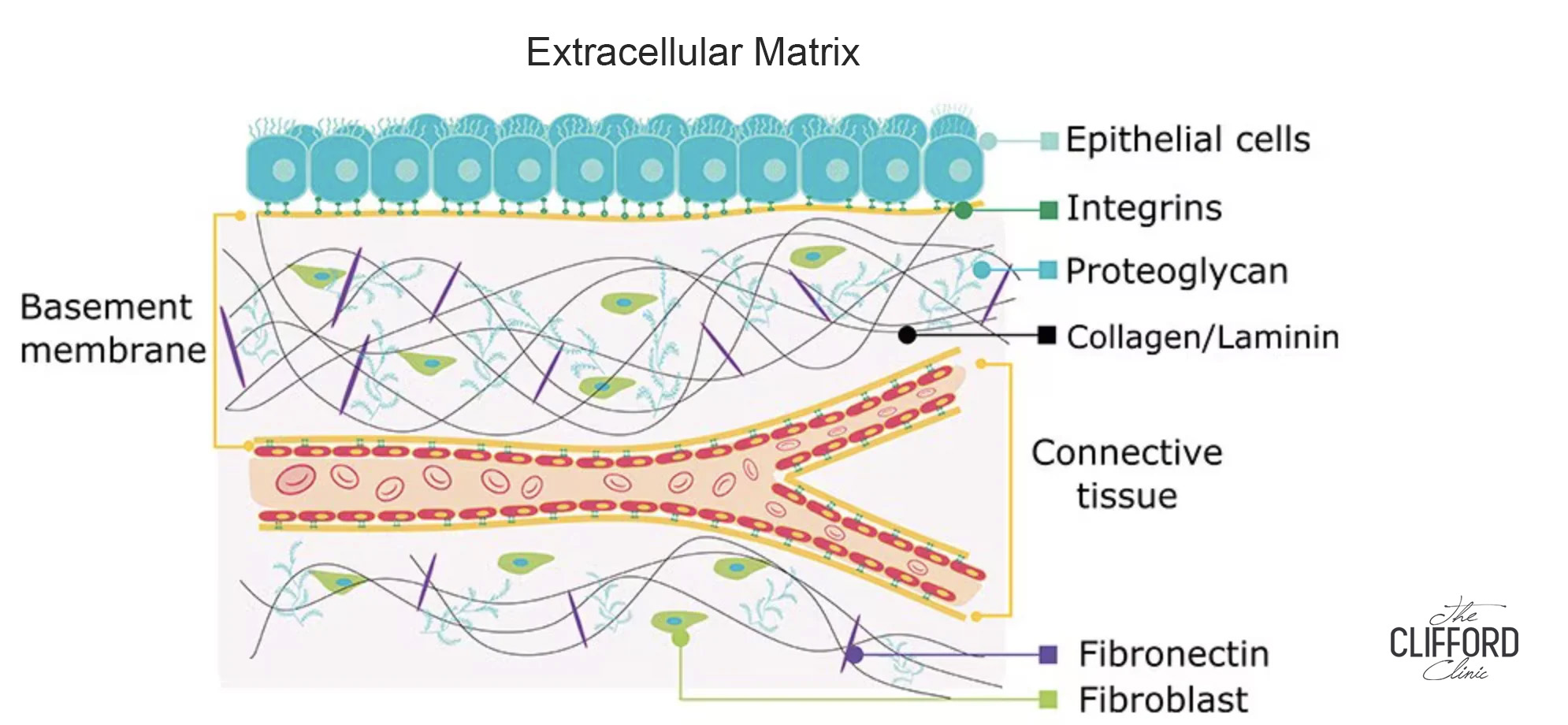
Any discussion of how skin rejuvenation treatments work has to begin with fibroblasts. These are the resident cells of the dermis, the deeper layer of skin beneath the epidermis, and they are responsible for producing virtually every structural component that gives skin its quality. Collagen, elastin, hyaluronic acid, fibronectin, laminin, glycosaminoglycans: all of these molecules originate from fibroblasts. When fibroblasts function well, skin functions well. When fibroblasts decline, skin ages.
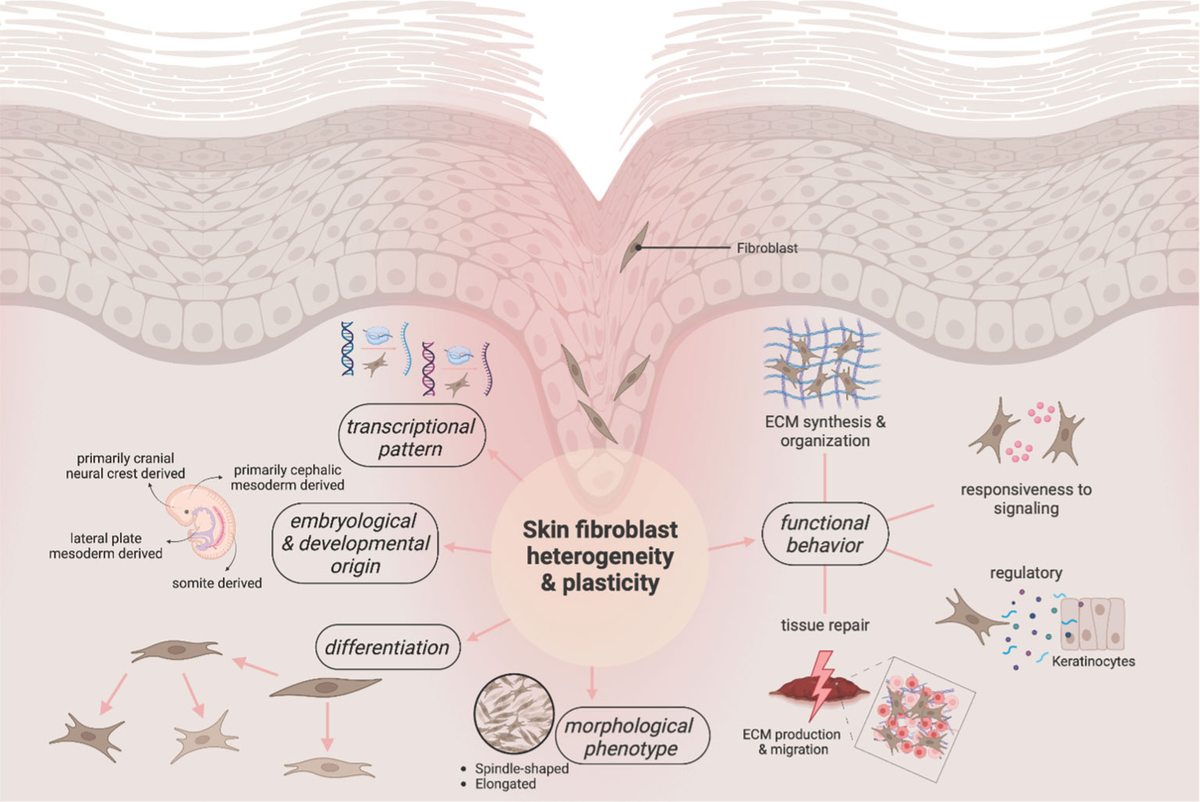
Fibroblasts have three primary roles in healthy skin. The first is structural support: synthesising extracellular matrix proteins that maintain tissue strength and architecture. The second is wound healing: releasing growth factors that coordinate tissue regeneration in response to injury. The third is inflammatory response regulation — secreting cytokines that modulate inflammation during repair. All three of these functions depend on fibroblasts being mechanically and biochemically stimulated by the matrix that surrounds them.
This last point is critical and often overlooked. Fibroblasts are not autonomous factories that produce ECM components on a fixed schedule. They are highly responsive cells that take constant cues from their environment. The ECM around a fibroblast tells it whether to proliferate, whether to produce collagen, whether to release growth factors, and whether to signal for new blood vessel formation. When the surrounding ECM is healthy, intact, and rich in mechanical signalling cues, fibroblasts are active and productive. When the ECM is fragmented, disorganised, or depleted, fibroblasts become quiescent, they essentially stop working at full capacity.
Why Ageing Skin Is Really a Problem of Fibroblast Quiescence
This is where the conventional understanding of skin ageing, that we lose collagen because we get older, becomes incomplete. The deeper truth is that we lose collagen because our fibroblasts are no longer receiving the structural and biochemical signals they need to keep producing it. Collagen production drops at approximately 1 to 1.5% per year from our twenties onward, but this is not because fibroblasts are failing in some intrinsic sense. It is because the ECM scaffold that supports them has begun to fragment, and they are responding to a less supportive environment by reducing their output.
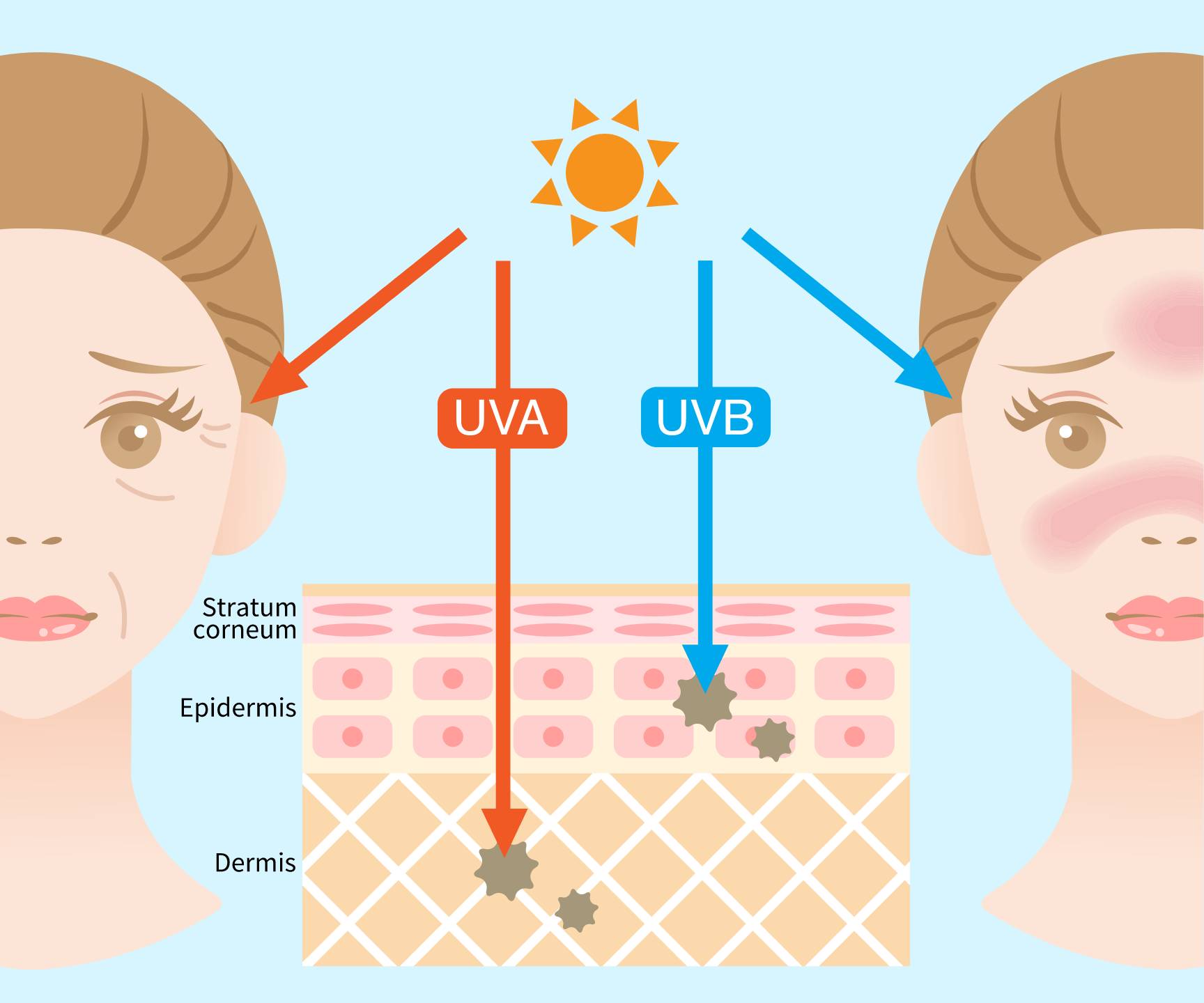
Sun exposure speeds this process up dramatically. Ultraviolet light damages the collagen and elastin fibres in the skin directly, leaving the matrix tangled and disorganised, what dermatologists call solar elastosis. At the same time, sunlight switches on a group of enzymes called matrix metalloproteinases, or MMPs, whose job is to break down old, worn-out collagen and elastin so that the fibroblasts can replace them. In sun-damaged skin, these enzymes work faster than the fibroblasts can rebuild, so the skin steadily loses its supportive scaffold. The fibroblasts sitting inside this fragmented scaffold are no longer surrounded by the structural cues they need to do their job properly, and their output of new collagen and elastin falls further still.
This insight reframes the goal of any meaningful skin rejuvenation treatment. It is not enough to add hydration to the skin’s surface, or to inject volume to mask wrinkles. To actually rejuvenate skin in a biologically meaningful way, you have to restore the ECM environment that fibroblasts depend on. This is precisely what Elravie Re2O is designed to do.
The Two Categories of Skin Booster: Stimulator vs Generator
Before exploring how Re2O works specifically, it is useful to draw a distinction that is now widely used in Korean and international aesthetic medicine literature: the difference between a stimulator and a generator.
A collagen stimulator is a product that signals fibroblasts to produce more of their own ECM. Hyaluronic acid skin boosters work this way, they stretch fibroblasts mechanically and create a hydrated environment that stimulates collagen production. Polynucleotide, also known as PDRN injections work similarly, providing biochemical signals that activate fibroblast metabolism. PDLLA and PCL are biodegradable polymers that act as foreign-body scaffolds, triggering an inflammatory-regenerative response that results in new collagen deposition. CaHA (calcium hydroxylapatite) products such as Radiesse work by similar principles. All of these are stimulators, they ask the skin to produce more.

An ECM generator, by contrast, directly supplies the ECM components themselves. Rather than asking the skin to produce more collagen and elastin, a generator delivers actual collagen, elastin, hyaluronic acid, and other matrix components directly into the dermis, where they integrate with existing tissue and provide the structural environment that fibroblasts need. Elravie Re2O is the first product in this category to use real human skin ECM, derived from acellularised donor dermal tissue.
The distinction matters because stimulators have a fundamental limitation: they depend on the residual capacity of fibroblasts to respond. In younger skin with relatively healthy fibroblast populations, stimulators work well. In significantly aged or photodamaged skin where fibroblast quiescence is more advanced, the response to stimulators diminishes. A generator, by contrast, does not depend solely on fibroblast capacity — it directly supplements the ECM regardless of how active the fibroblasts are, while simultaneously creating the conditions under which those fibroblasts can become active again.
| Expert Opinion — Dr Law Zhi Wei, Aesthetic Physician
“The stimulator-versus-generator framing is one of the clearest ways I can explain Re2O to a patient who has used skin boosters before. With stimulators, you are essentially negotiating with your existing fibroblast population — asking them, please make more. With Re2O, you are giving the skin the actual building blocks plus the structural environment that triggers fibroblasts to wake up. It is a fundamentally different conversation, and it is why I find Re2O particularly valuable in patients who have plateaued on other treatments. We are no longer relying on the skin’s diminishing capacity to respond. We are restoring the matrix, and the cellular response follows.”
|
 — Dr Law Zhi Wei, Aesthetic Physician, The Clifford Clinic Singapore
— Dr Law Zhi Wei, Aesthetic Physician, The Clifford Clinic SingaporeHow Re2O Is Made: The AlloClean Technology Process
Understanding how Re2O works at the tissue level requires first understanding how the product is produced. Elravie Re2O begins as donated human skin tissue, sourced from screened donors through tissue banking systems that meet the highest international regulatory standards. L&C Bio’s source materials are accredited by the AATB (American Association of Tissue Banks), FDA-listed for unprocessed tissue, and registered through Korea’s MFDS — the same regulatory frameworks that govern surgical tissue grafts used in reconstructive medicine.
From this starting tissue, L&C Bio applies its proprietary AlloClean Technology — a multi-stage decellularisation process that removes all cells, lipids, antigens, and pathogens from the dermal tissue while preserving the three-dimensional ECM architecture. This is the technological core of the product, and it is what distinguishes Re2O from competing approaches that either fail to fully decellularise the tissue (raising immunogenicity concerns) or that strip away ECM structure during processing (eliminating the biological activity that makes the product effective).
The result of AlloClean processing is a pure acellular dermal matrix that retains its native composition, collagen across multiple subtypes, elastin, glycosaminoglycans, fibronectin, laminin, tenascin, and bound growth factors while having no remaining cellular or genetic material that could trigger an immune response. Comparative assay data published by L&C Bio show residual DNA levels significantly below those of competing hADM processing platforms, providing an objective measure of decellularisation thoroughness.
The processed hADM sheet is then micronized into particles below 100 micrometres in diameter, fine enough to pass through standard aesthetic injection needles, while still large enough to retain the fibrous matrix architecture that signals fibroblast activity. This particle size is a critical engineering parameter: too small, and the matrix loses its structural cues; too large, and it cannot be evenly distributed through intradermal injection. Below 100 micrometres represents a deliberate balance point validated through clinical use.
The Dual-Function Mechanism: Immediate and Progressive Effects
Once Elravie Re2O is reconstituted — typically with normal saline, or with a non-crosslinked hyaluronic acid carrier such as RD-1 or Vital Light when added hydration is desired — and injected into the deep dermis, two distinct biological processes begin almost simultaneously. One produces immediate effects, the other unfolds progressively over weeks and months. This dual-function mechanism is central to understanding why patients see early results that continue to deepen over time, and it is supported by both preclinical and clinical work on injectable particulated human acellular dermal matrix (phADM) published by Kim and colleagues in 2026 in the International Journal of Molecular Sciences.
The Immediate Phase: Direct ECM Supplementation
The moment hADM particles enter the dermal tissue, the ECM components they contain are biologically active. Hyaluronic acid and other glycosaminoglycans within the matrix are powerfully hydrophilic, immediately binding water molecules and increasing tissue hydration at the injection site. The collagen fibrils within the matrix occupy interstitial space and provide a subtle micro-volumising effect that softens the appearance of fine lines, pores, and surface texture irregularities. Patients commonly notice a tangible improvement in skin smoothness and softness within the first 24 to 48 hours after treatment.
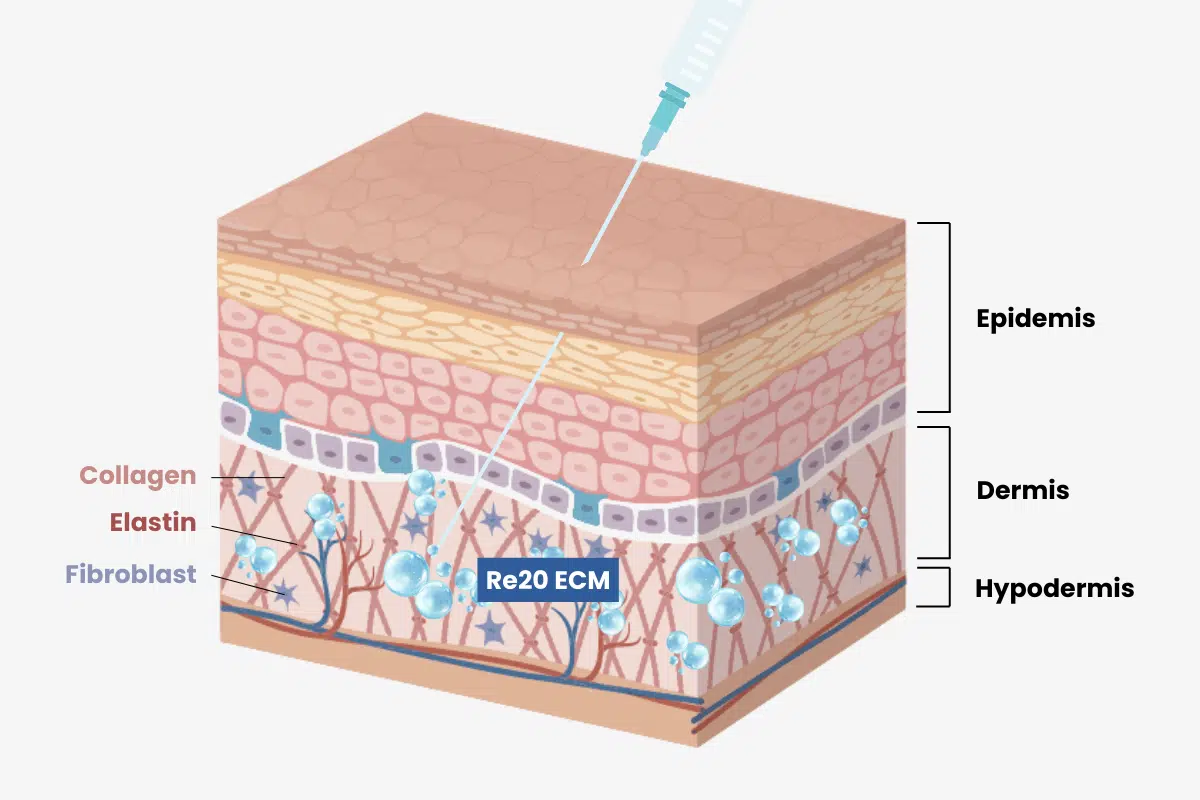
From the moment of injection, this freshly delivered ECM begins shaping the environment around the fibroblasts that live in the dermis. Whereas a synthetic filler or HA gel would primarily be displacing tissue, Re2O is actively restoring the matrix that those fibroblasts depend on to function — replacing what has been lost rather than simply taking up space.
The Progressive Phase: Fibroblast Activation and ECM Remodelling
Over the days and weeks that follow injection, a more complex cascade of biological events unfolds. Resident fibroblasts in the surrounding tissue migrate toward and incorporate themselves into the injected hADM scaffold. As they do so, they receive mechanical and biochemical signals from the matrix, exactly the signals that quiescent fibroblasts in aged tissue have been missing. These signals reactivate the fibroblasts and prompt them to begin producing new ECM components in earnest. In a rat model of intradermal phADM injection, Kim and colleagues observed pronounced fibroblast migration and a significant increase in fibroblast density within one week of injection, with the highest density of cells concentrated at the matrix–host interface where the implanted scaffold met the native dermis.
The result is a measurable increase in Type I collagen synthesis, Type III collagen synthesis, elastin production, and hyaluronic acid output. Fibroblast populations themselves expand as cell proliferation increases. Activated fibroblasts also begin secreting key growth factors, fibroblast growth factor (FGF) supports continued fibroblast proliferation and ECM synthesis; vascular endothelial growth factor (VEGF) drives the formation of new capillary blood vessels; insulin-like growth factor (IGF) and platelet-derived growth factor (PDGF) coordinate broader tissue regeneration; and transforming growth factor beta (TGF-β) regulates ECM remodelling and turnover. Each of these factors amplifies and extends the regenerative response well beyond the original injection. These mechanistic steps are not theoretical extrapolations: in vitro work on human dermal fibroblasts exposed to phADM has shown direct upregulation of collagen and elastin synthesis alongside increased VEGF, FGF and PDGF expression, and a separate study by Wang and colleagues demonstrated that porcine acellular dermal matrix induced human fibroblasts to secrete hyaluronic acid through activation of the JAK2/STAT3 signalling pathway, providing a molecular explanation for the hydration and matrix-rebuilding effects observed clinically.
Neovascularisation, the formation of new blood vessels, is a particularly important downstream effect. As VEGF stimulates new capillaries to form within the treatment area, the tissue becomes better perfused, with improved nutrient and oxygen delivery to fibroblasts and other dermal cells. This contributes to the gradual improvement in skin radiance and tone that patients report over the months following treatment, and it also creates a self-sustaining environment in which ECM regeneration continues long after the originally injected hADM has been remodelled and integrated.
Crucially, the original injected ECM does not simply persist as a foreign deposit. Over time, it integrates seamlessly with the newly synthesised ECM produced by activated fibroblasts. The injected matrix is gradually remodelled and replaced by new, native ECM — but the structural improvement persists, because the regenerative process has now become self-sustaining. The split-face randomised clinical trial reported by Kim and colleagues quantified this clinically: phADM-treated cheek skin showed significant improvements in skin density, volume and elasticity, with measurable reductions in wrinkle severity and pore size sustained through the 20-week follow-up period. This is consistent with what we see in our own practice — Re2O’s clinical effects continue for six months or more, and repeated treatments produce cumulative rather than additive benefits.
The Role of Particle Size and Injection Depth
Two technical parameters profoundly influence how well Re2O performs: particle size and injection depth. Both are worth understanding in detail, because they are areas where clinical technique directly affects clinical outcome.
Particle size below 100 micrometres allows the hADM material to be distributed evenly through fine intradermal injection while still presenting fibrous matrix surfaces large enough to support fibroblast attachment and incorporation. Particles much smaller than this would degrade more rapidly and provide less structural signalling. Particles much larger would tend to clump, produce visible lumps, or fail to integrate evenly. The L&C Bio specification of below 100 micrometres reflects extensive iteration to find the optimal balance. The importance of this particle range is supported by independent histological work: in studies of micronized cross-linked human acellular dermal matrix, Hsieh and colleagues showed that finely micronized ADM particles function as an effective three-dimensional scaffold for collagen synthesis, with progressive fibroblast infiltration and ordered new collagen deposition around the particles over the weeks following injection. Earlier work by Wu and colleagues on micronized ADM as a delivery vehicle for human fibroblasts likewise demonstrated that particles in this size range support fibroblast expansion and viability after intradermal placement.
Injection depth into the deep dermis, typically more than 2 millimetres below the skin surface, at an angle of 45 to 60 degrees — is equally important. The deep dermis is where fibroblast density is highest and where the existing ECM scaffold provides the best foundation for integration of injected hADM. Injection that is too superficial risks visible nodules and reduced biological effect, because the material cannot integrate properly into the dermal architecture. Injection that is too deep, into the subcutaneous fat layer, fails to deliver structural improvement to the dermis where it is needed. In the phADM clinical trial cited above, the investigators used an automated injection device specifically calibrated to target the mid-dermis in order to standardise depth and dosing, an acknowledgement that even within the published evidence base, depth accuracy is a determinant of outcome. A separate fluid-mechanics analysis of skin-booster injection by Cha and colleagues (2024) reinforced the point, showing that needle gauge, syringe diameter, viscosity of the reconstituted product and injection angle all measurably influence whether the bolus is deposited in the correct dermal plane. This is why Re2O is fundamentally a clinician-skill-dependent product: the molecule itself does what the science says it does, but only when it is placed precisely where it is supposed to go.
| Expert Opinion — Dr Law Zhi Wei, Aesthetic Physician
“One thing I cannot emphasise enough is how much practitioner skill matters with Re2O. Unlike a hyaluronic acid filler where the gel itself is forgiving and tends to produce reasonable results across a range of injection depths, Re2O is a true clinician-dependent product. The hADM particles need to be in the deep dermis, evenly distributed, and reconstituted to the right consistency for the area being treated. I have seen patients who tried Re2O elsewhere and were disappointed, only to have an excellent response when the technique was corrected. The product is genuinely capable of restoring the dermal matrix — but only when it is placed precisely where it needs to be. This is not a treatment to delegate to an inexperienced injector.” — Dr Law Zhi Wei, Aesthetic Physician, The Clifford Clinic Singapore |
How Re2O Compares Mechanistically to Other Skin Booster Categories
Placing Re2O’s mechanism alongside those of other skin booster categories highlights what makes the ECM generator approach distinctive.
Hyaluronic acid skin boosters such as Restylane Skinboosters and Profhilo work primarily through hydration and mild biostimulation. They draw water into the dermis, mechanically stretch fibroblasts, and stimulate a modest collagen response. Their effects are real but limited in depth, they replenish hydration and produce some collagen stimulation, but they do not address the broader ECM environment. Their duration of effect is typically three to six months.
PDRN-based products such as Rejuran work through a different pathway. Polynucleotide fragments derived from salmon DNA provide nucleotide-level signals that activate fibroblast metabolism, support DNA repair processes, and reduce inflammation. Rejuran is particularly well known for its anti-inflammatory and skin-quality effects, and for being well-tolerated in sensitive or rosacea-prone skin. However, like HA boosters, Rejuran is fundamentally a stimulator — it activates the skin’s own response without supplementing the structural ECM directly.

PDLLA and PCL collagen stimulators such as Sculptra, Juvelook, and certain newer Korean formulations use biodegradable polymer particles to trigger a controlled inflammatory-regenerative response. Macrophages encapsulate the polymer particles and recruit fibroblasts, which then deposit new collagen around the polymer scaffold. The effects can be substantial and long-lasting, often eighteen months or more but the mechanism is essentially indirect: the polymer is a foreign body that prompts a biological response, rather than a structural component the skin can directly use. There is also a more pronounced post-treatment inflammatory phase.
Calcium hydroxylapatite products such as Radiesse work through a similar foreign-body mechanism, providing both immediate volumising effect through the calcium microspheres themselves and progressive collagen stimulation as the spheres are gradually metabolised. CaHA is more commonly positioned as a deep volumiser with biostimulatory properties than as a skin booster per se.
Exosome-based treatments among the newer entrants to the category use cell-derived signalling vesicles to deliver biochemical cues that activate fibroblast and keratinocyte function. They are a powerful biological tool but again work through stimulation rather than ECM supplementation, and they do not provide a structural matrix for fibroblast incorporation.
Re2O occupies a categorically different position. By delivering real human skin ECM directly into the dermis, it both supplements the structural matrix and provides the mechanical and biochemical environment that activates fibroblasts. It is not competing with these other categories so much as it is operating on a different mechanistic axis — one that addresses the root problem of ECM degradation rather than the downstream consequence of reduced collagen synthesis. In clinical practice, this means Re2O can be effective in patients who have plateaued on stimulator-based treatments, and it can be combined with other modalities to achieve outcomes that no single approach delivers on its own.
Why the Source Tissue Matters: The Case for Real Human ECM
Across the global aesthetic injectable market, there are many products that claim to support collagen production. A patient might reasonably ask: if the goal is more collagen and elastin, why does it matter whether the source material is human, porcine, bovine, fish, or fully synthetic? The answer lies in the principle of biocompatibility and biological mimicry.
Human skin ECM has a specific composition that human fibroblasts evolved to recognise. The proportions of Type I, III, IV, V, VI, VII, and XVII collagen, the specific architecture of elastin fibres, the ratio of glycosaminoglycans to structural proteins, and the bound growth factors retained within the matrix all reflect millions of years of co-evolution between fibroblasts and the matrix they inhabit. When fibroblasts encounter human ECM in their environment, they receive precisely the signals they expect, and they respond in physiologically appropriate ways.
Porcine collagen, bovine collagen, fish collagen, and synthetic collagens approximate this signalling but do not replicate it exactly. They can produce useful clinical effects, but they also carry varying degrees of immune compatibility risk, and their structural cues do not match native human tissue with the same fidelity. Synthetic polymers are even further removed as their effects depend on triggering an inflammatory-regenerative response rather than providing biologically authentic signals.
Re2O’s use of real human skin ECM, fully decellularised but structurally preserved, eliminates these compatibility concerns. The matrix is biologically identical to what already exists in the patient’s own dermis, only fresh and intact rather than fragmented and aged. There is no immune rejection risk, no foreign-body response, and no compromise in signalling fidelity. This is why Re2O is described — accurately, in our view — as the first injectable that genuinely returns to the skin what the skin has lost.
The Cumulative Effect: Why Multiple Sessions Build on Each Other
One of the more subtle but clinically important features of Re2O’s mechanism is that the effects of repeated treatments are cumulative rather than simply additive. Understanding why requires returning to the fibroblast biology described earlier.
After the first Re2O session, fibroblasts are activated, new ECM is synthesised, and the dermal scaffold begins rebuilding. This regenerative environment persists for weeks to months, and in many patients it represents a significant improvement over their baseline state. When a second session is performed approximately four weeks later, it does not simply add another layer of effect on top of the first. Instead, it builds upon a tissue environment that is already biologically more active than it was at baseline. Fibroblasts that have been recently activated respond more vigorously to additional matrix supplementation. The newly synthesised ECM from the first session integrates with the freshly injected hADM, creating a progressively richer scaffold.
By the third session, the cumulative effect on dermal density, fibroblast activity, and matrix richness is substantially greater than would be predicted from simply adding the effects of three independent treatments. This is the biological rationale for the standard three-session loading protocol, and it is also why patients often describe their results after the full course as qualitatively different from what they noticed after the first session alone — not just more, but better in a different way.
Maintenance treatments every six to nine months serve to refresh this regenerative environment before fibroblast activity has fully returned to its previous baseline. Done consistently over time, this approach can shift the trajectory of skin ageing not by stopping it altogether, but by repeatedly intervening at the matrix level to keep fibroblasts active and the ECM scaffold supported.

What This Means for Patients Considering Re2O
Bringing all of this together, what should a patient considering Elravie Re2O take away from the science? A few key points stand out.
First, Re2O works because it addresses the actual biological problem of skin ageing, ECM degradation and fibroblast quiescence rather than just managing symptoms at the surface. This is a meaningful distinction from most other injectables on the market, and it is the basis of the durability and depth of the clinical response.
Second, the immediate effects of Re2O are real but they are only the beginning. The most important changes are the activation of fibroblasts, the synthesis of new collagen and elastin, the formation of new blood vessels, and the rebuilding of dermal density that develop over weeks and months following treatment. Patients who expect a single-session, instantaneous result will be better served by other treatments. Patients who are willing to commit to a structured course and a medium-term outcome will see Re2O at its best.
Third, the quality of the result depends heavily on injection technique. Re2O is not a forgiving product in the way some HA fillers are. Its effects are greatest when it is placed precisely in the deep dermis, evenly distributed, and reconstituted appropriately for the treatment area. Choosing an experienced clinician who understands the product’s mechanism and has refined their technique through clinical practice is essential.
Finally, Re2O can be combined intelligently with other treatments. Energy-based devices such as fractional radiofrequency or non-ablative laser create additional fibroblast activation that synergises with the ECM supplementation provided by Re2O. Non-crosslinked HA can be incorporated into the Re2O preparation for enhanced hydration. Other regenerative treatments such as PRP or exosomes can complement the ECM-level approach. A skilled clinician will integrate Re2O into a broader plan tailored to your specific skin and goals.
| The Clifford Clinic — Our Approach to Re2O
At The Clifford Clinic, we view Elravie Re2O as one of the most important advances in injectable aesthetic medicine in the past decade — but we also believe that the science only translates into real outcomes when the treatment is delivered with care, precision, and clinical judgement. Dr Law Zhi Wei takes time to understand the biological state of each patient’s skin before recommending a Re2O protocol. For some patients, Re2O alone will deliver excellent results. For others, it is most effective when integrated into a broader programme that may include energy-based devices, complementary injectables, or topical regenerative therapies. If you are interested in understanding whether Elravie Re2O is right for your skin, we invite you to book a consultation with Dr Law at The Clifford Clinic, Singapore. |
References
- Landau M, Fagien S. Science of Hyaluronic Acid Beyond Filling: Fibroblasts and Their Response to the Extracellular Matrix. Plastic and Reconstructive Surgery. 2015.
- Widgerow AD, Fabi SG, Palestine RF, et al. Extracellular Matrix Modulation: Optimizing Skin Care and Rejuvenation Procedures. Journal of Drugs in Dermatology. 2016.
- Cui Y, Wang F, Voorhees JJ, Fisher GJ. Rejuvenation of Aged Human Skin by Injection of Cross-Linked Hyaluronic Acid. Plastic and Reconstructive Surgery. 2021.
- Hsieh DM, Bi X, Zhong S, Wu Y. In Vivo Investigation of the Biostimulatory and Rejuvenating Effects of Small-Particle Cross-Linked Hyaluronic Acid Injections in Photoaged Human Skin. Aesthetic Surgery Journal. 2023.
- Stellavato A, Corsuto L, D’Agostino A, et al. Hyaluronan Hybrid Cooperative Complexes as a Novel Frontier for Cellular Bioprocesses Re-Activation. PloS One. 2016.
- Kim YH, Park S, Cho JH, Han SY, Cho SW. Multifunctional Skin Dermal Extracellular Matrix Enabling Skin-Relevant Bioactivity for Tissue Remodeling, Hydration, and Anti-Hyperpigmentation. Journal of Microbiology and Biotechnology. 2026.
- Park S, Lee MJ, Kim HJ, et al. Skin ECM Provides a Bio-Derived Platform for Supporting Dermal Renewal and Matrix Synthesis. Journal of Microbiology and Biotechnology. 2025.
- Widgerow AD, Markowitz O, Carruthers J, Jacob C, Robison T. Dermatoporosis: Strategies for Rebuilding the Extracellular Matrix of the Skin. Journal of Drugs in Dermatology. 2023.
- Smith L, Rahmati M, Pizzol D, et al. Biostimulants in Aesthetic Medicine: A Systematic Review and Meta-Analysis of Efficacy, Safety, and Patient Satisfaction. Aesthetic Surgery Journal. 2025.
- Fisher SM, Borab Z, Weir D, Rohrich RJ. The Emerging Role of Biostimulators as an Adjunct in Facial Rejuvenation: A Systematic Review. Journal of Plastic, Reconstructive and Aesthetic Surgery. 2024.
- L&C Bio. Elravie Re2O Training Slide — Confidential Product Documentation. L&C Bio Co. Ltd., South Korea. 2024.
- Kim YH, Park S, Cho JH, et al. Injectable Particulated Human Acellular Dermal Matrix Booster for Skin Restoration: An Integrated Randomized, Split-Face, Double-Blinded Clinical Trial and Preclinical Study. International Journal of Molecular Sciences. 2026;27(5):2193.
- Hsieh DM, Bi X, Zhong S, Wu Y. Micronized Cross-Linked Human Acellular Dermal Matrices: An Effective Scaffold for Collagen Synthesis and Promising Material for Tissue Augmentation. Aesthetic Surgery Journal Open Forum. 2018.
- Wu Y, Wang J, Shi Y, et al. Expansion and Delivery of Human Fibroblasts on Micronized Acellular Dermal Matrix for Skin Regeneration. Biomaterials. 2009;30(8):1486–1494.
- Wang Q, Zhang J, Sun Y, et al. A Porcine Acellular Dermal Matrix Induces Human Fibroblasts to Secrete Hyaluronic Acid by Activating JAK2/STAT3 Signalling. Journal of Cellular and Molecular Medicine. 2022.
- Cha S, Lee J, Park H, et al. Investigating the Mechanisms of Intradermal Injection for Easier “Skin Booster” Treatment: A Fluid Mechanics Approach to Determine Optimal Delivery Method. Skin Research and Technology. 2024.