



Treatment of Alopecia Areata in Singapore: UVB, Dovobet, Fraxel 1927 & Bellasonic for Diffuse Alopecia Areata
Diffuse alopecia areata is one of the most easily missed forms of autoimmune hair loss. Unlike classic alopecia areata, which usually appears as sharply defined round patches, diffuse alopecia areata can look more like generalized thinning, excessive shedding, or a sudden drop in hair density across the scalp. That is why many patients in Singapore initially assume they have stress-related shedding, telogen effluvium, or female pattern hair loss when the real issue is immune-mediated. Alopecia areata is a non-scarring autoimmune disorder that affects about 1.7% to 2% of the population, and diffuse presentations are part of its clinical spectrum.
For treatment of Alopecia Areata, the key message is simple: diagnosis comes first, and treatment only works well when it matches the biology of the disease. In diffuse alopecia areata, the aim is not just to “stimulate hair growth.” The real aim is to reduce immune attack on the follicle, support the hair cycle back into anagen, improve the scalp environment, and use delivery systems that help topical agents reach the right level of the scalp. That is where narrowband UVB, topical calcipotriol, Dovobet, Fraxel 1927 thulium laser, and Bellasonic can enter the conversation. The evidence is strongest for Ultraviolet B and calcipotriol-based therapy, while Fraxel 1927 and Bellasonic are better framed as adjunctive tools in a broader scalp strategy.
What is diffuse alopecia areata?
Alopecia areata is a common, non-scarring hair loss disorder in which the immune system mistakenly targets the hair follicle. The disease can affect the scalp, beard, eyebrows, eyelashes, or body hair. In diffuse cases, instead of seeing only one or two obvious patches, patients may notice widespread thinning, more scalp visibility, or rapid shedding that seems out of proportion to normal hair fall. The British Association of Dermatologists notes that alopecia areata can sometimes present with hair loss that is “spread out,” and the clinical review literature also recognizes a diffuse variant with widespread thinning across the scalp.
That distinction matters because diffuse alopecia areata can look deceptively similar to telogen effluvium. In practice, careful diagnosis usually depends on history, scalp examination, trichoscopy, hair-pull findings, and pattern recognition. Exclamation-mark hairs, short tapered hairs, sudden onset, relapsing behavior, nail changes, and autoimmune associations can all point toward alopecia areata rather than ordinary shedding.
Pathophysiology: why alopecia areata happens
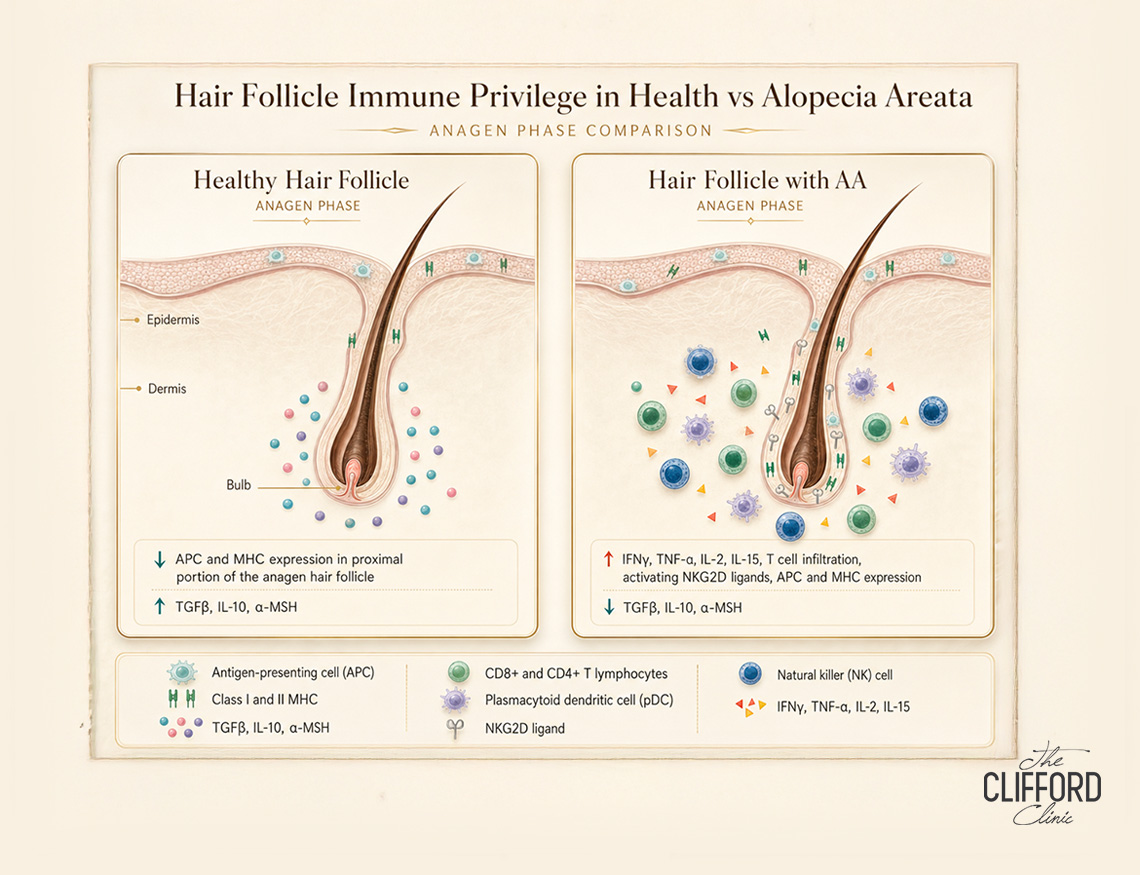
The pathophysiology of alopecia areata is centered on a collapse of hair-follicle immune privilege. Under normal conditions, the growing follicle partly protects itself from immune surveillance. In alopecia areata, that protection breaks down. CD8-positive and CD4-positive lymphocytes, interferon-related signaling, and other inflammatory mediators then begin to target the anagen follicle, disrupting the hair cycle and triggering shedding. Histologically, classic alopecia areata shows a peribulbar lymphocytic infiltrate often described as a “swarm of bees.”
Vitamin D biology may also be relevant. Recent reviews emphasize that vitamin D and the vitamin D receptor are involved in follicular immune privilege, keratinocyte regulation, and hair-follicle homeostasis. Vitamin D deficiency is frequently reported in alopecia areata cohorts, and altered VDR signaling has been linked with increased disease severity, longer duration, and higher relapse risk in some studies, although not every study has shown the same strength of association. This is one reason calcipotriol-based therapy and Ultraviolet B (UVB) therapy attract interest: both intersect with the vitamin D pathway, although they do not act in identical ways.
Disease progression, duration, and outcomes
One reason patients search so urgently for the Treatment of Alopecia Areata is that the course of the disease is unpredictable. Hair can regrow on its own over months and, more rarely, over years, but this cannot be guaranteed and new patches can occur in the future. Prognosis is better when less hair is lost at the beginning, while extensive hair loss carries a lower chance of full recovery.
Published prognosis estimates vary depending on the population studied. An older but still widely cited review reported that about 34% to 50% of patients recover within a year, while roughly 14% to 25% may progress to alopecia totalis or universalis. Some may have complete regrowth within a year without treatment, but outcomes are much worse when more than half the scalp is involved or when complete scalp loss develops. Younger age at onset, nail involvement, ophiasis-pattern disease, family history, and concomitant autoimmune disease are all associated with poorer prognosis.
This is why the treatment of Alopecia Areata is often best understood as disease control plus regrowth support, rather than a one-off “fix.” Even when hair returns, relapse remains common. Patients frequently need follow-up, photography, reassessment at the 2- to 3-month mark, and sometimes step-up or combination therapy.
Treatment of Alopecia Areata: why UVB deserves attention
Narrowband UVB is one of the more overlooked non-surgical options in alopecia areata. Its relevance is not simply that “light helps hair.” The more useful explanation is that UVB has immunomodulatory effects and may help alter the inflammatory environment around the follicle. In broader phototherapy literature, NB-UVB is known to induce apoptosis of pathogenic T lymphocytes and reduce inflammatory signaling. In AA-specific literature, monochromatic UVB-based therapy is described as decreasing cytokine production via T-cell apoptosis.
The strongest directly relevant trial here is the randomized controlled study by El Taieb and colleagues, which compared topical calcipotriol, NB-UVB, both together, and placebo in 60 patients with scalp alopecia areata over 3 months. All active treatment groups showed significant SALT-score improvement, while the placebo arm did not. NB-UVB and calcipotriol both improved SALT score and vitamin D3 levels, and the combination increased vitamin D3 more than either monotherapy, though it was not clearly superior to either single treatment in clinical SALT improvement. That makes UVB a reasonable non-invasive option for selected scalp cases, especially when the goal is an immune-modulating, steroid-sparing clinic treatment.
The important nuance is that NB-UVB is not universally effective in every alopecia areata patient. In severe AA, earlier data were less encouraging. One study of patients with severe disease reported that NB-UVB was not especially effective, with only 20% achieving an excellent response. The practical takeaway is that UVB may be more useful in limited, localized, or selected scalp disease than in the most severe end of the spectrum.
Treatment of Alopecia Areata: topical calcipotriol and Dovobet
Topical calcipotriol is a vitamin D analogue with plausible biologic relevance in alopecia areata. It influences keratinocyte differentiation, immune signaling, and vitamin D receptor pathways in the follicle. A 2025 systematic review and meta-analysis concluded that vitamin D3 and its analogues may serve as a safe, inexpensive option for mild-to-moderate patchy alopecia areata, either alone or as an adjunct. Across 496 cases using vitamin D3 or its analogues, the pooled overall success rate in mild-to-moderate AA was reported as 53.75%, though the authors also noted heterogeneity and limited trial quality.
The calcipotriol literature is stronger for patchy or localized AA than for diffuse AA specifically, but it is still relevant. In a pilot intrasubject study of 35 patients with scalp AA, calcipotriol 0.005% ointment showed greater and faster response than topical clobetasol, although differences were not statistically significant; the authors concluded that calcipotriol appeared reasonably effective for mild-to-moderate patchy AA with limited and reversible side effects. In the randomized UVB trial, topical calcipotriol twice daily for 12 weeks also produced significant SALT-score improvement compared with baseline and placebo.
Now to the important point about Dovobet. Strictly speaking, Dovobet is not calcipotriol alone. It is a fixed combination of calcipotriol plus betamethasone dipropionate; in some countries the same combination is marketed as Daivobet. Official product information lists it as a psoriasis medication, which means using it for alopecia areata is off-label and should be medically supervised.
That said, there is published AA data on the combination. In a 2023 randomized controlled trial, 60 patients with chronic localized alopecia areata were assigned to topical tacrolimus 0.03%, Daivobet (topical potent steroid plus vitamin D analogue), or clobetasol 0.05% for 3 months with 3 more months of follow-up. The Daivobet group produced results comparable to clobetasol, with lower values in a non-statistically significant way and fewer side-effect concerns; tacrolimus performed worst. The study concluded that the vitamin D analogue plus potent steroid combination appeared more convenient than a superpotent steroid because of comparable efficacy and fewer side effects. That is meaningful support for Dovobet/Daivobet as a calcipotriol-based topical option, but it is still fair to say the best published evidence remains in localised rather than truly diffuse AA.
Other treatment options in the Treatment of Alopecia Areata
Current guidance and dermatologist resources still position topical corticosteroids and intralesional corticosteroid injections as mainstream first-line tools, especially for limited scalp disease. The AAD notes that injections every 4 to 6 weeks are often the most effective option for a few patches, and topical corticosteroids are also commonly used, particularly in children.
For more extensive disease, clinicians may consider contact immunotherapy, systemic immunosuppressive agents, or JAK inhibitors. The AAD currently notes that three JAK inhibitors are FDA-approved in the United States for alopecia areata: baricitinib for adults with severe AA, deuruxolitinib for adults with severe AA, and ritlecitinib for adults and adolescents aged 12 and older with extensive hair loss. These options matter most in more severe or extensive disease, but they sit outside the narrow focus of this article, which is diffuse AA and conservative or clinic-based adjunctive care.
The treatment options we offer: Fraxel 1927 thulium laser

At The Clifford Clinic, Fraxel 1927 thulium laser is one of the available hair-loss treatments that improves scalp quality, blood flow, and topical penetration. A PubMed-indexed split-scalp study evaluated the therapeutic efficacy and safety of a 1927-nm fractionated thulium laser in pattern hair loss, and broader reviews of laser-assisted drug delivery in alopecia conclude that fractional lasers can enhance penetration of scalp medications and improve overall results in some alopecia settings.
In resistant alopecia areata, published case series show benefit from fractional laser-assisted topical triamcinolone and from fractionated CO2 laser plus topical tacrolimus 0.1%, supporting the broader principle that energy-assisted delivery can enhance penetration of immune-active topicals.
Bellasonic: LDM, scalp delivery, and immune-modulating topicals

Bellasonic, a Local Dynamic Micro-Ultrasound (LDM) and ultrasound device, can improve blood flow, oxygenation, and the delivery of topical hair serums or medications through cavitation bubbles. Reviews on ultrasound-mediated transdermal drug delivery and low-frequency sonophoresis describe ultrasound as a non-invasive method that can significantly increase skin permeability and enhance transdermal transport. Experimental work has also shown that ultrasound plus microbubble cavitation can enhance scalp delivery of hair therapeutics such as minoxidil. That makes Bellasonic a reasonable adjunctive delivery platform in a hair clinic setting.
For diffuse alopecia areata, Bellasonic can help support a customised scalp program by improving penetration of growth-factor serums, nutrients, and selected topical medications.
Why Dr Gerard Ee’s background matters
When patients are evaluating the Treatment of alopecia areata in Singapore, experience matters because diffuse hair loss is easy to misclassify. Dr Gerard Ee is an ARTAS-certified robotic hair restoration surgeon, trained at St George’s University of London, worked at SGH, NUH, and Mount Sinai Hospital in New York, and obtained Membership of the Royal College of Surgeons (Edinburgh) plus a postgraduate diploma in dermatology.
As Dr Gerard Ee writes in his hair-restoration commentary, “I recommend a two-pronged approach of a hair transplant in conjunction with follow up treatments.” In the context of diffuse alopecia areata, that same combination mindset is useful even when surgery is not the answer: diagnose precisely, choose the correct core therapy, and then add the right adjuncts to support regrowth and scalp recovery.
Realistic treatment timelines and outcomes
Patients usually do better when expectations are set properly. Hair regrowth takes time, even when a treatment is working. In the calcipotriol-versus-NB-UVB trial, the primary assessment point was 12 weeks, and that is a useful clinical benchmark for conservative AA treatments. AAD guidance on patchy AA likewise notes that when corticosteroid injections are effective, some regrowth is usually seen within about 3 months of the first treatment.
In milder disease, patients may recover spontaneously or respond to topicals, UVB, or injections. In more persistent or extensive disease, treatment often becomes layered, longer-term, and more individualized.
FAQ
Is diffuse alopecia areata the same as telogen effluvium?
No. Telogen effluvium is usually a hair-cycle shift after stress, illness, or other triggers. Diffuse alopecia areata is immune-mediated and can mimic telogen effluvium visually, which is why proper scalp diagnosis matters.
Does UVB really work for alopecia areata?
It can work in selected patients. In the randomized trial comparing calcipotriol, NB-UVB, combination therapy, and placebo, all active arms improved while placebo did not. However, older data suggest NB-UVB is less reliable in severe AA.
Is Dovobet the same as calcipotriol?
Not exactly. Dovobet is a combination of calcipotriol and betamethasone dipropionate. In alopecia areata, that makes it different from calcipotriol-only studies, and its use for AA is off-label.
Can Fraxel 1927 thulium laser treat diffuse alopecia areata by itself?
The best way to describe it is as an adjunct. The strongest direct 1927-nm evidence is in pattern hair loss, while broader alopecia literature supports energy-assisted drug delivery as a useful add-on rather than a definitive standalone cure for AA.
Can Bellasonic help deliver growth factors, steroids, or Protopic into the scalp?
The clinic describes Bellasonic as an ultrasound/LDM platform that improves delivery of topical hair serums and medications through cavitation and enhanced absorption. Ultrasound-assisted transdermal delivery is scientifically plausible, but Bellasonic-specific AA data remain limited, so this is best seen as a medically supervised adjunctive strategy.
References
-
El Taieb MA, Hegazy EM, Ibrahim HM, Osman AB, Abualhamd M. Topical calcipotriol vs narrowband ultraviolet B in treatment of alopecia areata: a randomized-controlled trial. Arch Dermatol Res. 2019. PubMed summary: . Uploaded full text:
-
BAD patient information leaflet on alopecia areata, including prognosis, recurrence, and diffuse presentations.
-
BAD living guideline plain-language summary for alopecia areata 2024.
-
Darwin E, et al. Alopecia Areata: Review of Epidemiology, Clinical Features, Pathogenesis, and New Treatment Options.
-
Jiménez-Herrera EA, et al. Vitamin D and Alopecia Areata: From Mechanism to Therapeutic Implications.
-
Alsaati AA, et al. Vitamin D and its Analogs in Treatment of Mild to Moderate Alopecia Areata: Systematic Review and Meta-Analysis.
-
Molinelli E, et al. Efficacy and Safety of Topical Calcipotriol 0.005% Versus Topical Clobetasol 0.05% in the Management of Alopecia Areata.
-
Nassar A, et al. Comparative evaluation of topical tacrolimus 0.03% and topical calcipotriol 0.005% mixed with betamethasone dipropionate versus topical clobetasol 0.05% in treatment of alopecia areata.
-
Official Dovobet / Daivobet drug information confirming it is a calcipotriol-betamethasone product indicated for psoriasis, not alopecia areata.
-
AAD treatment overview for alopecia areata, including corticosteroids, contact immunotherapy, minoxidil, and JAK inhibitors.
-
Laser and energy-assisted delivery literature for alopecia, plus AA case series using topical triamcinolone or tacrolimus with fractional laser.
-
1927-nm fractionated thulium laser study in pattern hair loss.
-
Ultrasound-mediated transdermal delivery literature supporting the scientific basis for ultrasound-enhanced penetration.