



Why Melasma Needs “Low-Heat, Long-Game” Treatment: How Lorient Element Skin Booster can help
Melasma is one of those skin conditions that teaches patients an uncomfortable lesson: the harder you “attack” it, the more it can push back. In Singapore, where daily UV exposure is high and heat is part of life, melasma pigmentation and uneven skin tone often behave like a chronic, relapsing condition rather than a one-time spot you can erase.
That is why the most reliable approach is usually not a single aggressive session, but a low-heat, long-game plan that reduces pigment production, lowers inflammation and supports the skin barrier over time.
Within that kind of plan, Lorient Element Skin Booster is positioned as a skin booster that focuses on a small set of brightening and barrier-supporting ingredients, typically used alongside controlled energy-based treatments and a consistent home routine.
What is Lorient Element Skin Booster?
Lorient Element is an energy-based device (EBD) booster designed to support melasma pigmentation and uneven skin tone by pairing a simple, focused formula with in-clinic delivery methods. Instead of combining many ingredients, it is built around a small set of actives commonly used in pigmentation management, such as tranexamic acid, niacinamide, vitamin C (ascorbic acid) and glutathione, along with a hyaluronic acid-based vehicle (including acetylated hyaluronic acid) to support hydration and skin comfort.
The concept is “minimally maximum,” meaning fewer components but higher functional intent, with a focus on brightening support while reducing unnecessary additives that can trigger irritation in sensitive, pigment-prone skin.
In practice, Lorient Element is typically used as part of a longer-term melasma strategy rather than a one-off brightening session. It is positioned to complement controlled, low-heat treatment plans because melasma often worsens with excessive inflammation and thermal stress.
By supporting antioxidant defence, pigment signalling control and barrier hydration, Lorient Element is commonly integrated into programmes where consistency matters, especially for patients who flare easily, relapse after sun or heat exposure, or struggle with uneven tone that does not respond well to topical skincare alone.
Why melasma responds poorly to “high heat”
Melasma is not just pigment sitting on the surface. It is a pigment disorder driven by multiple triggers and heat and inflammation are two of the most important. Many patients notice their melasma worsens after sun exposure, hot yoga, long outdoor walks, cooking over heat, or even after certain laser sessions that create too much thermal load. This does not mean lasers are “bad.” It means melasma is sensitive to the way energy is delivered.
Melasma tends to flare when the skin is repeatedly pushed into a stressed state. Heat can amplify inflammatory signals in the skin and inflammation can activate pigment pathways. Once the pigment “machine” is switched on, it becomes harder to calm down quickly.
That is why many effective melasma plans use a lower-heat approach, spread out over time, with strict attention to UV and barrier stability. The goal is not to shock pigment into submission. The goal is to quiet the pigment system and keep it quiet.
The pigment biology that makes melasma stubborn
To understand why melasma is so persistent, it helps to understand what pigment cells do. The key cell is the melanocyte, often described as the cell responsible for producing melanin. Melanocytes do not just “make pigment once.” They respond continuously to signals from UV, hormones, inflammation and skin injury.
In practice, melasma is often driven by a mix of factors:
- UV and visible light exposure, which increases pigment signalling and oxidative stress.
- Hormonal influences, especially in women, include pregnancy and oral contraceptives in certain individuals.
- Inflammation and skin irritation, which can come from friction, harsh skincare, heat-based procedures, or barrier breakdown.
- Vascular and dermal changes, which can make pigment behaviour more complex and relapse more likely.
This is why melasma is often called “chronic.” The triggers do not disappear after one treatment. They persist in daily life, especially in Singapore.
Epidermal vs dermal vs mixed melasma
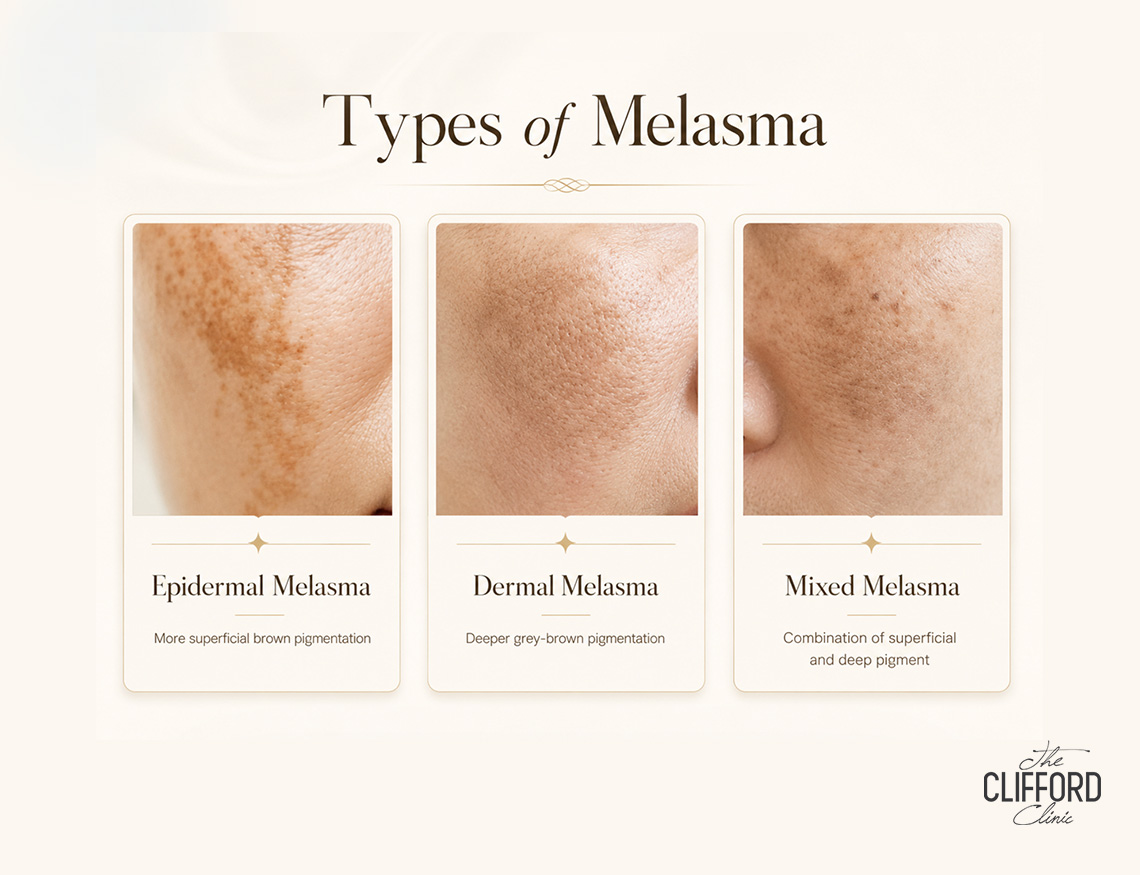
Melasma can be described as predominantly epidermal, dermal, or mixed, depending on where pigment is distributed. This distinction matters because it influences how quickly results appear and how likely relapse is.
When pigment is mainly epidermal, improvement can sometimes be faster with appropriate topical strategies and controlled energy treatments. When pigment extends deeper or behaves more like a dermal inflammatory condition, treatment often needs to be gentler and longer-term. In many real-world cases, melasma is mixed.
This is one reason “spot treatment thinking” often fails. Melasma is not always a single layer problem, so it rarely responds like one.

What “low-heat, long-game” actually means in clinic terms
A low-heat, long-game melasma plan typically means:
- Avoiding excessive thermal injury that can inflame the skin and trigger rebound pigmentation.
- Using controlled, lower-intensity energy-based sessions where appropriate, spaced out with enough recovery time.
- Supporting pigment control biochemically using targeted ingredients that act on melanocyte activation, melanin production, pigment transfer, oxidative stress and inflammation.
- Building a strict daily prevention routine, because UV and visible light exposure can undo progress.
The long-game part is not about “slow treatment.” It is about stable treatment. Many patients in Singapore prefer a plan that produces steady improvement with fewer setbacks, rather than quick improvement followed by a flare.
Where Lorient Element fits in this strategy
Lorient Element is typically discussed as a skin booster used for melasma pigmentation and uneven skin tone support, especially when you want to combine brightening ingredients with a delivery method that makes sense clinically.
Rather than mixing many actives, Lorient Element’s concept is to keep the formula focused and rely on a handful of commonly discussed pigment-modulating ingredients.
At a practical level, it is used as part of a broader plan that still includes UV discipline, barrier repair and careful treatment sequencing. It does not replace all melasma management steps. It is one component that can be layered into a plan where inflammation control and pigment signalling control are priorities.
The 5 “roles” a melasma product ideally covers
When you look at melasma as a system problem, you start to see why single-ingredient solutions can be incomplete. A comprehensive approach usually needs to address at least five roles:
- Reduce melanocyte overactivation
- Reduce melanin production signals
- Reduce pigment transfer to surface skin cells (where it becomes visible)
- Reduce oxidative stress and inflammation
- Support barrier and hydration, because barrier disruption fuels inflammation and pigment relapse
The reason a low-heat approach matters is that heat and inflammation can undo multiple steps above at once.
Why delivery matters more than most people realise
A Singapore-friendly treatment rhythm
In many melasma plans, clinic sessions are spaced out every few weeks, with the “work” happening in between sessions as the skin remodels and pigment signalling quiets down. Patients often do best with:
- consistent UV and visible light protection daily
- steady, tolerable brightening support
- controlled in-clinic sessions at sensible intervals
- ongoing monitoring so intensity can be adjusted before flares occur
This rhythm matters in Singapore because melasma triggers are not occasional. They are daily.
Pairing Lorient Element with laser treatments
Lorient Element is often positioned as an adjunct in programmes that involve controlled energy-based treatments, because lasers can improve uneven skin tone by targeting pigment at different depths, but melasma needs a more conservative approach than “spot blasting.”
Pairing a measured laser plan with pigment-modulating and barrier-supporting care helps the skin settle and stabilise between sessions, rather than cycling into irritation that makes melasma darker.
Clinics may use pigment-targeting options such as a pico laser for pigmentation or a Q-switch laser for pigmentation when the goal is to break up excess pigment carefully and gradually. For patients whose melasma behaves more like a long-term uneven tone issue with textural components, controlled resurfacing and tone support may also be discussed using a fractional approach such as the Fraxel Dual laser, again with cautious parameters and longer spacing where appropriate.
The exact choice depends on whether pigmentation is more epidermal, dermal, or mixed and whether the skin is reactive, inflamed, or prone to post-inflammatory darkening.
The overall pairing strategy is usually not “laser alone,” but “laser plus stabilisation.” That means a plan that includes strict sun protection, avoidance of overheating triggers and supportive in-clinic steps that reduce pigment signalling and improve tolerance so you can stay consistent for the long term. For a broader overview of how pigmentation is approached and how different devices are selected, you can refer to your clinic’s pigmentation page and then discuss melasma-specific precautions and sequencing in consultation.
What results should look like if the plan is working
Melasma improvement is often subtle at first. You may notice:
- less “darkening after sun”
- a reduction in patch contrast rather than complete disappearance
- a more even tone in certain lighting
- fewer flare cycles
This is a better early sign than expecting the patch to vanish quickly. A melasma plan is doing its job when the skin becomes more stable and less reactive to triggers. Once stability improves, progressive tone improvement becomes easier to maintain.
What can derail results, even with good treatment
In Singapore, the most common reasons melasma relapses even after improvement include:
- inconsistent sunscreen use or inadequate reapplication
- reliance on “brightening” products that irritate the skin
- overheating triggers (sun, hot environments, certain procedures)
- stopping maintenance abruptly after improvement
- treating melasma like a spot rather than a long-term condition
This is why the “low-heat, long-game” idea is practical rather than theoretical. It is designed around how melasma behaves in real life.
Who tends to be a good candidate for Lorient Element

In general, Lorient Element is most relevant when a patient’s main concern is melasma pigmentation and uneven skin tone, especially when:
- the skin is sensitive and cannot tolerate aggressive routines
- pigment relapses after heat or irritation
- the patient is already doing sunscreen but still sees persistent patches
- a combined plan with devices and pigment support is being considered
Suitability still depends on your skin type, pigment depth, trigger profile and tolerance. A structured assessment matters.
Practical home routine principles that support the “long-game”
No in-clinic plan survives daily UV exposure without a stable home routine. For melasma in Singapore, the foundations usually include:
- daily broad-spectrum sunscreen and sensible reapplication habits
- avoidance of skin irritation from harsh scrubs, over-exfoliation, or aggressive “brightening” layering
- consistent barrier support, especially if using actives
- reducing heat triggers where practical, such as prolonged direct sun exposure
The goal is not perfect behaviour. The goal is reducing repeated flares.
Closing perspective
Melasma is best treated like a chronic condition that needs stability, not like a stain that needs a one-time scrub. A low-heat, long-game approach recognises that melasma pigmentation and uneven skin tone are driven by melanocyte behaviour, inflammation, oxidative stress and daily environmental triggers, especially in Singapore.
Within that strategy, Lorient Element can be used as a focused skin booster option to support pigment control and barrier stability, particularly when combined thoughtfully with prevention and, when appropriate, carefully selected in-clinic energy-based treatments.
If you are planning your next step, it often helps to start with a structured consult that clarifies whether your melasma behaves more epidermal, dermal, or mixed and then builds a plan around your specific triggers.
FAQs
1) Why does melasma often worsen with “too much heat,” even if the laser is technically targeting pigment?
Melasma is not purely a pigment deposit problem. Heat can amplify inflammatory signalling, oxidative stress and vascular mediators that keep melanocytes active and increase melanin transfer. When the skin is pushed into repeated thermal stress, the risk is rebound pigmentation, especially in mixed or dermal-pattern melasma. A low-heat approach aims to reduce cumulative inflammation so pigment control becomes more stable over time.
2) If my melasma lightens, why does it come back so easily in Singapore?
Melasma tends to relapse because the drivers remain present: UV exposure, visible light, heat and hormonal or inflammatory triggers. Even after visible pigment improves, the “pigment signalling environment” can still be primed, so small triggers create a flare. Long-term maintenance is usually about preventing reactivation rather than chasing perfect clearance in one cycle.
3) If Lorient Element uses actives under 500 Daltons, why does delivery still matter?
Molecular size is only one barrier. Skin permeability also depends on the stratum corneum integrity, formulation pH, charge state (especially relevant for tranexamic acid) and whether the skin is inflamed or overly dry. Controlled, clinic-based delivery windows (for example after specific energy-based treatments) can improve uptake without forcing you to use harsh daily routines that inflame the barrier and worsen melasma.
4) How should Lorient Element be sequenced with lasers to reduce rebound pigmentation risk?
Most melasma plans do better with pre-conditioning and conservative spacing. This often means stabilising barrier and pigment signalling first, then using carefully selected laser parameters and repeating at longer intervals rather than frequent “high-impact” sessions. Many clinicians also prioritise strict photoprotection and avoid stacking multiple heat-based treatments too close together, because cumulative inflammation is a common reason for relapse.
References
- Bos JD, Meinardi MM. The 500 Dalton rule for the skin penetration of chemical compounds and drugs. Exp Dermatol. 2000;9(3):165–169.
- Espósito ACC, Cassiano DP, da Silva CN, et al. Update on Melasma—Part I: Pathogenesis. Dermatol Ther (Heidelb). 2022;12:1967–1988. doi:10.1007/s13555-022-00779-x.
- Mekawy KM, Sadek A, Seddeik Abdel-Hameed AK. Microneedling versus fractional carbon dioxide laser for delivery of tranexamic acid in the treatment of melasma: a split-face study. J Cosmet Dermatol. 2021;20(2):460–465.
- Wanitphakdeedecha R, Sy-Alvarado F, Patthamalai P, et al. Thulium 1927-nm fractional laser-assisted topical tranexamic acid delivery for facial melasma: a split-face, double-blind, randomized controlled pilot study. Lasers Med Sci. 2020;35:2015–2021.
- Pazyar N, Raeispour M, Yaghoobi R, Seyedtabib M. Microneedling with tranexamic acid vs microneedling with vitamin C in melasma: a prospective single-blind trial. Health Sci Rep. 2023;6(10):e1636.
- Iraji F, Nasimi M, Asilian A, et al. Mesotherapy with tranexamic acid and ascorbic acid with and without glutathione in melasma: a split-face comparative trial. J Cosmet Dermatol. 2019;18(5):1416–1421.
- Wohlrab J, Kreft D. Niacinamide—mechanisms of action and its topical use in dermatology. Skin Pharmacol Physiol. 2014;27(6):311–315.
- Hakozaki T, Minwalla L, Zhuang J, et al. The effect of niacinamide on reducing cutaneous pigmentation and suppression of melanosome transfer. Br J Dermatol. 2002;147(1):20–31.
- Hakozaki T, Takiwaki H, Miyamoto K, Sato Y, Arase S. Ultrasound enhanced skin-lightening effect of vitamin C and niacinamide. Skin Res Technol. 2006;12(2):105–113.
- Greatens A, Hakozaki T, Koshoffer A, et al. Effective inhibition of melanosome transfer to keratinocytes by lectins and niacinamide is reversible. Exp Dermatol. 2005;14(7):498–508.
- Meunier M, Scandolera A, Chapuis E, et al. Anti-wrinkle properties of sodium acetylated hyaluronate. J Cosmet Dermatol. 2022;21(7): 2749 –2762.
- Handog EB, Datuin MSL, Singzon IA. Safety and efficacy of a novel preparation of glutathione as a skin-lightening agent in Filipino women: an open-label trial. Int J Dermatol. 2016;55(2):153–157.
- Goo BL. Laser assisted drug and cosmeceutical delivery system of the skin. Med Lasers. 2015;4(2):51–59.
- Hantash BM, Bedi VP, Sudireddy V, et al. Laser-induced transepidermal elimination of dermal content by fractional photothermolysis. J Biomed Opt. 2007;12(3):034008.
- Ablon G. Fractional laser resurfacing for the treatment of melasma: a review with special consideration to treatment in skin of color. J Clin Aesthet Dermatol. 2016;9(7):31.