


Hyperbaric Oxygen for Wounds: The Clinical Evidence
Wound healing is the most thoroughly researched and the most firmly established application of hyperbaric medicine. Hyperbaric oxygen for wounds is a recognised treatment for specific non-healing wounds supported by decades of clinical evidence. This guide explains how it works, which wounds respond to hyperbaric oxygen therapy (HBOT), and what the research shows. For the wider picture, please see our complete guide to hyperbaric oxygen therapy.
Why Some Wounds Will Not Heal
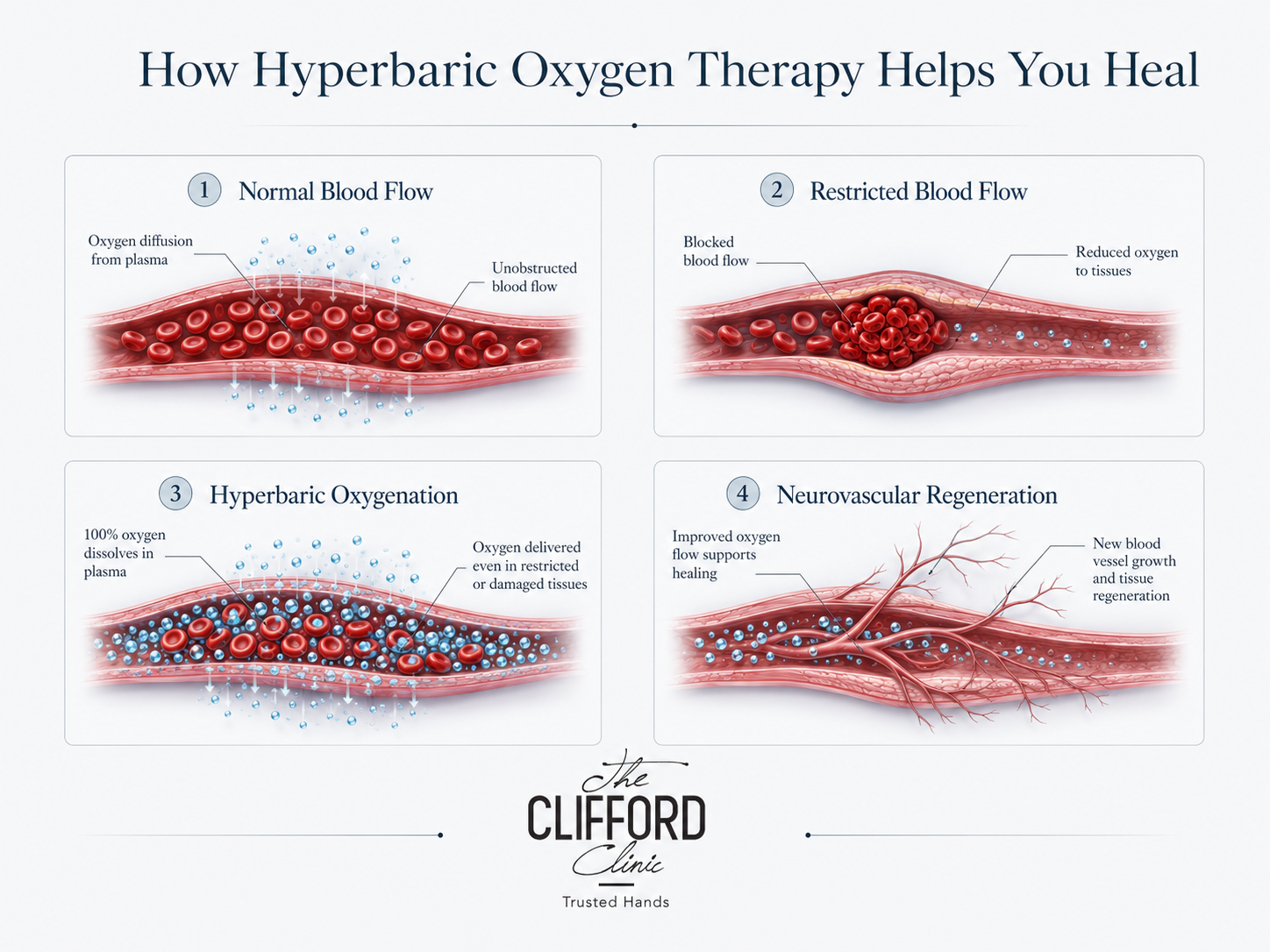
Wound healing is an oxygen-dependent process. To close a wound, the body needs oxygen to fight infection, build new blood vessels, lay down collagen and rebuild the skin surface.
When tissue oxygen falls too low, peripheral arterial disease or after radiation damage, the healing process stalls and the wound stays open regardless of dressings or antibiotics. Diabetic microvascular disease is an example of a condition that causes lack of oxygen in tissue.
Low tissue oxygen levels are the root cause of wounds staying open. As Bhutani and Vishwanath explained in their 2012 review in the Indian Journal of Plastic Surgery, hyperbaric oxygen therapy directly addresses this by raising tissue oxygen to levels ordinary breathing cannot reach.
How Hyperbaric Oxygen Heals Wounds
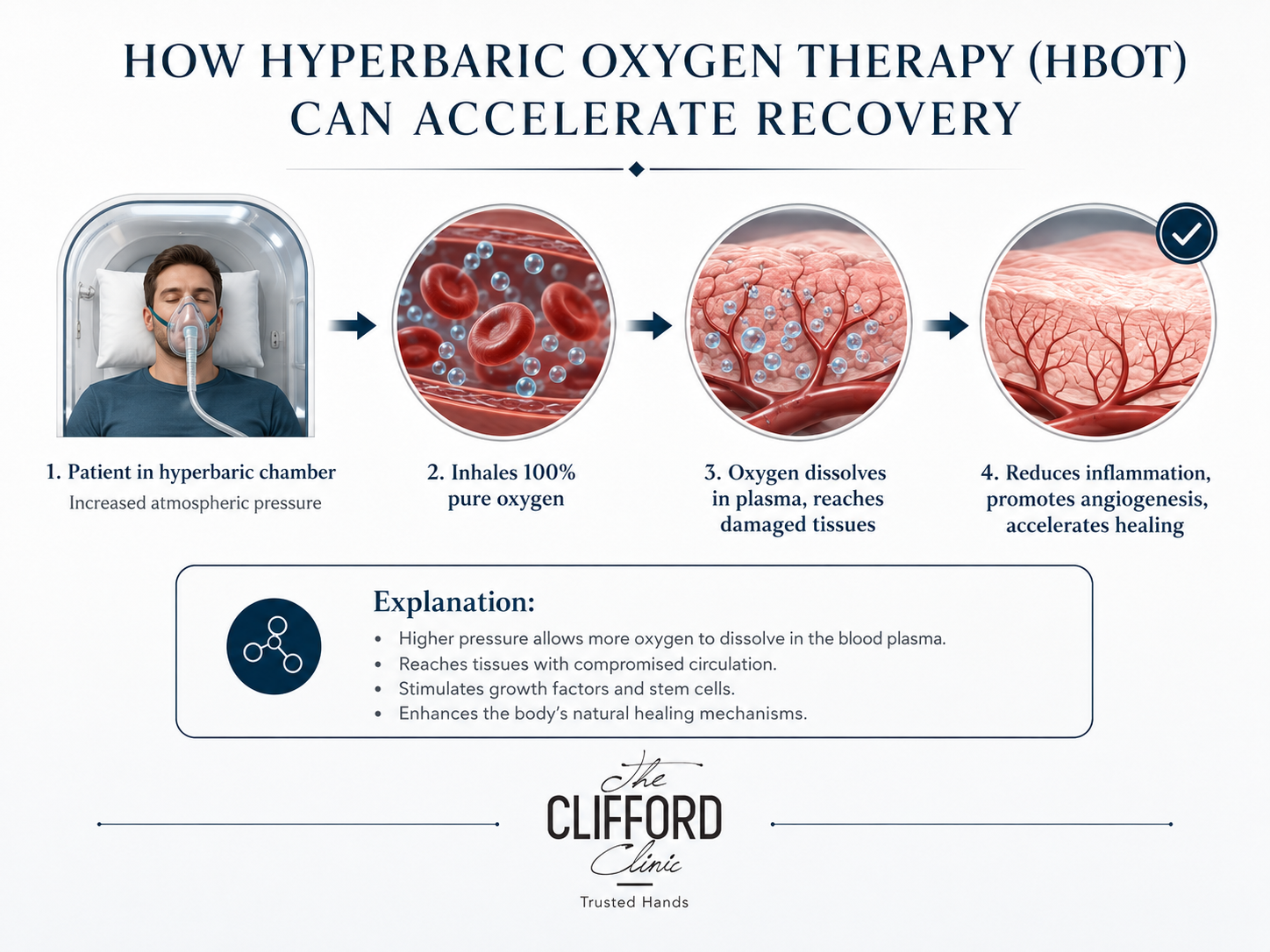
The 2009 Journal of Applied Physiology review by Stephen Thom gives a clear account of the wound-healing mechanism. Thom’s analysis was organized around processes where controlled clinical trials have demonstrated HBOT’s efficacy and wound healing ability prominently. The mechanisms include:
- Hyperoxygenation restores the oxygen gradient wounds need to heal.
- Angiogenesis builds new capillaries. The 2010 Godman study in Cell Stress and Chaperones showed HBOT directly enhances new vessel formation in human vascular cells.
- Stem cell mobilisation. Thom’s work showed that HBOT recruits CD34-positive progenitor cells that support tissue regeneration.
- Antimicrobial action. High oxygen levels are directly hostile to anaerobic bacteria and improve the ability of white blood cells to kill pathogens.
- Anti-inflammatory modulation helps break the chronic inflammation cycle that keeps wounds open.
Diabetic Foot Ulcers
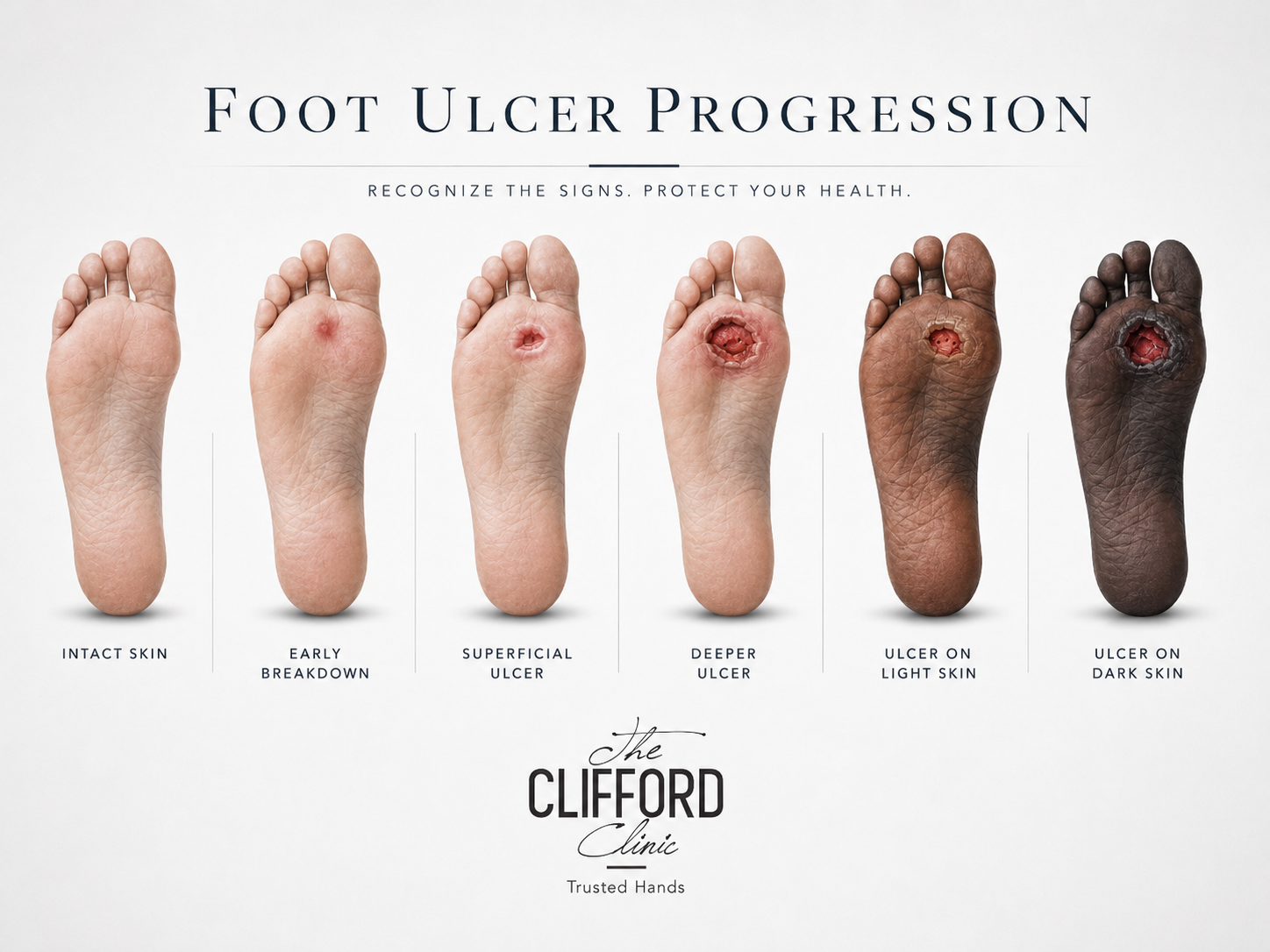
Diabetic foot ulcers are the most studied wound indication for HBOT, and one of the 14 indications formally approved by the Undersea and Hyperbaric Medical Society.
Patients with diabetes face a combination of nerve damage, poor circulation and impaired immunity which can lead to the formation of diabetic foot ulcers. As these factors also impair healing, a foot ulcer can quickly progress toward amputation. Clinical literature shows that HBOT, used alongside proper wound care, can improve healing rates in advanced diabetic foot ulcers and shift outcomes toward saving the limb.
Serious Infections: The Fournier’s Gangrene Evidence
The benefits of using HBOT for wound and infection care was demonstrated in the 2015 review published in Acta Médica Portuguesa by Rosa and Guerreiro. The team reviewed 34 cases of a severe necrotising infection known as Fournier’s gangrene that were referred for hyperbaric oxygen therapy over a 25-year period at a naval hyperbaric centre.
The patients were majority male, with a mean age of around 54. Diabetes was the most frequently associated condition with the patients which the authors highlighted as a likely predisposing factor for developing Fournier’s gangrene.
Fournier’s gangrene can be rapidly fatal. Despite the severity of this infection the mortality rate of the patients was around 21%, which is low for this dangerous condition. Hyperbaric oxygen, when used alongside surgical debridement and antibiotics, improved the survival rate because high oxygen levels are both bactericidal and supportive of tissue survival.
Other Wounds That Respond to HBOT
- Radiation tissue injury including osteoradionecrosis and soft tissue radionecrosis after cancer radiotherapy.
- Compromised skin grafts and flaps at risk of failing.
- Crush injuries and acute traumatic ischaemia.
- Necrotising soft tissue infections. HBOT can be used as a secondary therapy to surgery and antibiotics.
- Chronic non-healing wounds such as venous and pressure ulcers when standard care has failed.
HBOT Is an Adjunct, Not a Replacement
Hyperbaric oxygen for wounds works best alongside proper wound management such as debridement, offloading pressure, infection control and, for diabetic patients, glycaemic control. HBOT can be used as a secondary therapy or to restart a stalled healing, but wound management must still be practiced.

The Wound Healing Timeline With HBOT
Wound healing with hyperbaric oxygen is gradual, measured in weeks. In the early sessions the work is largely invisible as oxygen is still reaching previously starved tissue and the stalled healing cascade is just restarting. Over the following weeks, angiogenesis builds new capillaries and measurable changes in wound size and tissue quality will be visible. Most wound care protocols run 30 to 60 near-daily sessions in a hard-shell hyperbaric oxygen chamber. Consistency is essential because an interrupted course undermines the body’s cumulative biological response to HBOT.
Preventing Wound Recurrence
Closing a wound is only half of the overall treatment goal. For patients with diabetes or vascular disease, the underlying conditions that causes the patient to wound easily still remain.
Hyperbaric oxygen for wounds works best when paired with longer-term prevention. Good glycaemic control, appropriate footwear, vascular review and regular skin checks are vital for wound prevention. At The Clifford Clinic, wound-focused HBOT can be coordinated with wider longevity and health services, such as health screenings, that can help identify the conditions behind slow healing.
The Diabetic Foot Ulcer Evidence in Depth
Diabetic foot ulcers are the most studied HBOT wound indication. Diabetic foot ulcers are caused by a cascade of issues. Diabetes damages small blood vessels and nerves, which reduces oxygen delivery and blunts the warning signal of pain. A minor injury thus escalates into an ulcer. As the ulcer cannot heal because the tissue is starved of oxygen, an infection then sets in.
Hyperbaric oxygen interrupts this cascade at its root by raising tissue oxygen to levels ordinary circulation cannot achieve. The 2009 Journal of Applied Physiology review by Stephen Thom catalogued the wound-healing mechanisms involved from angiogenesis to enhanced antimicrobial defence. Used alongside debridement, offloading and glycaemic control, HBOT is a recognized and approved treatment for advanced diabetic foot ulcers. The end goal in these cases were HBOT is used to support healing is the prevention of amputation.
Radiation Injury: A Distinct Wound Problem
Not all difficult wounds are caused by diabetes. Patients who have had radiotherapy for cancer can develop radiation tissue injury months or years post-therapy as the treated tissue slowly loses its blood supply. This includes osteoradionecrosis, where the jawbone is affected after head and neck radiation therapy, and soft tissue radionecrosis.
Radiation injury is one of the formally approved indications for HBOT. Godman and colleagues showed in their 2010 laboratory studies that HBOT can rebuild the blood supply that radiation destroyed through the angiogenic mechanisms.
Crush Injuries and Acute Wounds
Not every wound that benefits from HBOT is a slow or chronic one. Hyperbaric oxygen also has an established role in acute trauma treatment, particularly for crush injuries and the acute traumatic ischaemia that can follow them.
In a crush injury, swelling raises pressure within the tissue which chokes off the blood supply and starves the area of oxygen at exactly the moment it is most needed. Hyperbaric oxygen interrupts this destructive loop. By dissolving oxygen directly into the plasma, HBOT delivers oxygen to tissue that swelling has cut off from the normal circulation. This was shown in the 1996 New England Journal of Medicine review by Tibbles and Edelsberg.
When used early, HBOT can reduce tissue death and improve long-term function. This acute role sits alongside its more familiar chronic-wound applications reinforcing that HBOT is most valuable wherever a healing process has stalled for lack of oxygen.
The Bottom Line on HBOT for Wounds
Hyperbaric oxygen for wounds is one of the most firmly evidenced uses of the therapy. It works by restoring the oxygen to wounds that have stalled their healing. HBOT works best alongside proper wound care rather than instead of it. For patient such as those who face a non-healing diabetic ulcers, HBOT can be the difference between healing and a far worse outcome.

The Clifford Clinic Perspective
When it comes to using Hyperbaric oxygen for wound care, The Clifford Clinic’s clinical team speaks from direct hands-on experience rather than just literature alone. As The Clifford Clinic is also an accredited Day Surgery Centre, the team frequently see and handles surgical wounds on top of chronic ulcers, and HBOT is used by the team to treat both types of wounds.
A significant part of the team’s work is post-surgical. The clinical team uses hyperbaric oxygen for wounds and tissue that need help recovering after an operation, both to support healing and to reduce the swelling that follows. The clinic has experience treating a wide range of patients including paediatric patients after surgery. Cases they handle range from secondary closure of wound to finger reattachment. Team regards HBOT as genuinely important in the treatment of all these different types of cases and patients.
For example, for a finger reattachment case, the survival of the repaired nerve, blood vessels and soft tissue depends heavily on those tissues receiving enough oxygen while circulation is still fragile, and that is precisely what hyperbaric oxygen delivers.
The clinical team would like to emphasize, however, that HBOT is an adjunct. It works alongside good surgical technique, wound care and medical management, not instead of them. In the team’s experience over four years and more than 200 patients, hyperbaric oxygen as an adjunct for wound care can meaningfully improve outcomes. When used correctly, HBOT closes wounds faster and in reattachment and compromised-tissue cases, raises the survival rate.
The team’s guiding principle is that screening by a SHUMEC-accredited doctor is the key for a proper diagnosis and treatment protocol should always be built around the diagnosis. When paired with medical knowledge and used as a part of a wider treatment plan, the team feel that HBOT has earned its place in wound care.
Frequently Asked Questions
Does hyperbaric oxygen really heal wounds?
Yes, for specific non-healing wounds. It is a recognised, approved treatment for advanced diabetic foot ulcers, radiation tissue injury and compromised grafts, used alongside standard wound care.
How many HBOT sessions does a wound need?
Most wound protocols involve 30 to 60 sessions usually delivered daily for five days per week.
Can HBOT help with serious infections?
Yes, as an adjunct. The 2015 Fournier’s gangrene review showed that can be HBOT used alongside surgery and antibiotics in severe necrotising infections.
Can HBOT prevent amputation?
For certain diabetic foot ulcer patients, HBOT can improve healing and shift outcomes toward limb salvage when combined with comprehensive wound care.
Key Research References
- Bhutani S, Vishwanath G. Hyperbaric oxygen and wound healing. Indian Journal of Plastic Surgery, 2012.
- Thom SR. Oxidative stress is fundamental to hyperbaric oxygen therapy. Journal of Applied Physiology, 2009.
- Godman CA et al. Hyperbaric oxygen induces a cytoprotective and angiogenic response in human microvascular endothelial cells. Cell Stress and Chaperones, 2010.
- Rosa I, Guerreiro F. Hyperbaric Oxygen Therapy for the Treatment of Fournier’s Gangrene: A Review of 34 Cases. Acta Medica Portuguesa, 2015.
To discuss a wound-healing assessment, book a consultation at The Clifford Clinic.